Ewy Gordon A
Department of Medicine (Cardiology) University of Arizona College of Medicine Tucson AZ USA.
Acute Med Surg. 2017 May 26;4(3):227-234. doi: 10.1002/ams2.281. eCollection 2017 Jul.
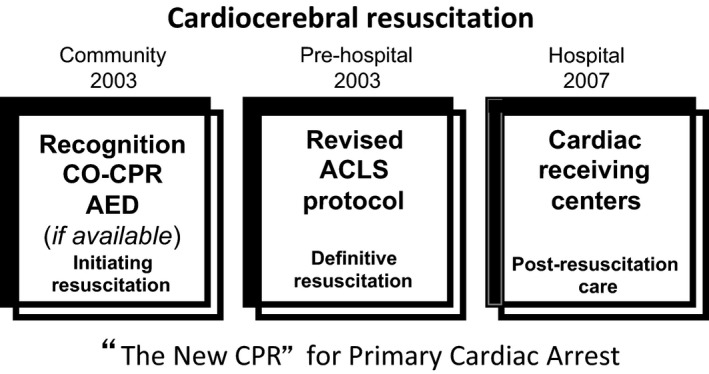
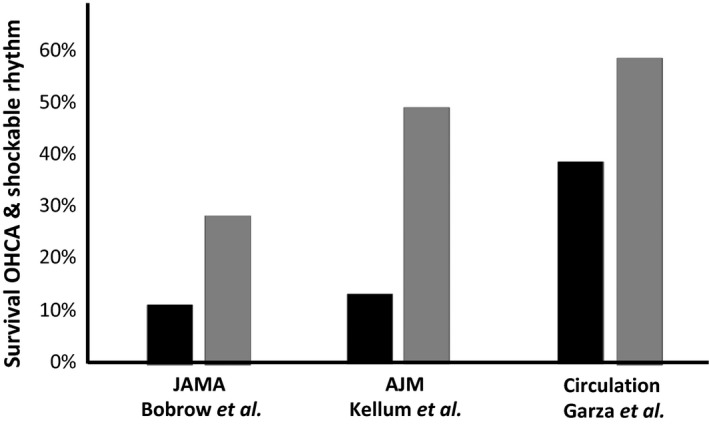
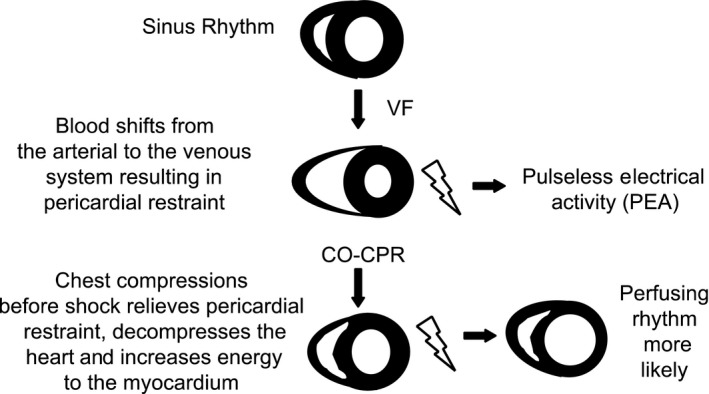
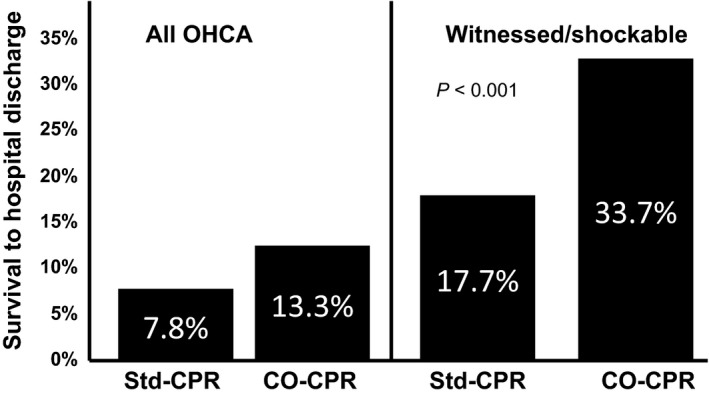
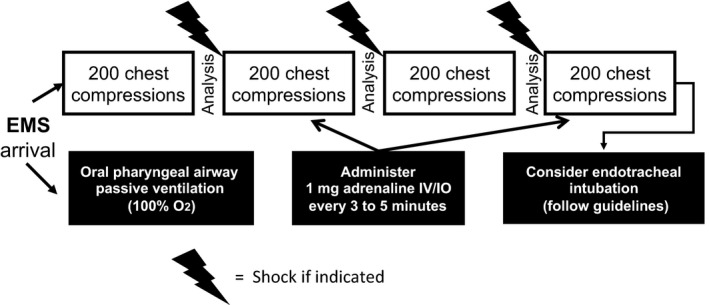
Sudden cardiac arrest is a major public health problem in the industrialized nations of the world. Yet, in spite of recurrent updates of the guidelines for cardiopulmonary resuscitation and emergency cardiac care, many areas have suboptimal survival rates. Cardiocerebral resuscitation, a non-guidelines approach to therapy of primary cardiac arrest based on our animal research, was instituted in Tucson (AZ, USA) in 2002 and subsequently adopted in other areas of the USA. Survival rates of patients with primary cardiac arrest and a shockable rhythm significantly improved wherever it was adopted. Cardiocerebral resuscitation has three components: the community, the pre-hospital, and the hospital. The community component emphasizes bystander recognition and chest compression only resuscitation. Its pre-hospital or emergency medical services component emphasizes: (i) urgent initiation of 200 uninterrupted chest compressions before and after each indicated single defibrillation shock, (ii) delayed endotracheal intubation in favor of passive delivery of oxygen by a non-rebreather mask, (iii) early adrenaline administration. The hospital component was added later. The national and international guidelines for cardiopulmonary resuscitation and emergency medical services are still not optimal, for several reasons, including the fact that they continue to recommend the same approach for two entirely different etiologies of cardiac arrest: primary cardiac arrest, often caused by ventricular fibrillation, where the arterial blood oxygenation is little changed at the time of the arrest, and secondary cardiac arrest from severe respiratory insufficiency, where the arterial blood is severely desaturated at the time of cardiac arrest. These different etiologies need different approaches to therapy.
心脏骤停是世界工业化国家的一个重大公共卫生问题。然而,尽管心肺复苏和紧急心脏护理指南不断更新,但许多地区的生存率仍不理想。心脑复苏是一种基于我们动物研究的原发性心脏骤停治疗的非指南方法,于2002年在美国亚利桑那州图森市实施,随后在美国其他地区采用。无论在何处采用,原发性心脏骤停且心律可电击复律患者的生存率都显著提高。心脑复苏有三个组成部分:社区、院前和医院。社区部分强调旁观者识别和仅进行胸外按压的复苏。其院前或紧急医疗服务部分强调:(i)在每次指示的单次除颤电击前后紧急开始200次不间断胸外按压,(ii)延迟气管插管,优先采用非重复呼吸面罩被动给氧,(iii)早期给予肾上腺素。医院部分是后来添加的。由于多种原因,包括它们继续对两种完全不同病因的心脏骤停推荐相同方法,即原发性心脏骤停(通常由室颤引起,心脏骤停时动脉血氧合变化不大)和严重呼吸功能不全导致的继发性心脏骤停(心脏骤停时动脉血严重低氧),心肺复苏和紧急医疗服务的国家和国际指南仍不理想。这些不同病因需要不同的治疗方法。