Bogousslavsky J, Miklossy J, Regli F, Janzer R
Department of Neurology, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
J Neurol Neurosurg Psychiatry. 1990 Jan;53(1):67-71. doi: 10.1136/jnnp.53.1.67.
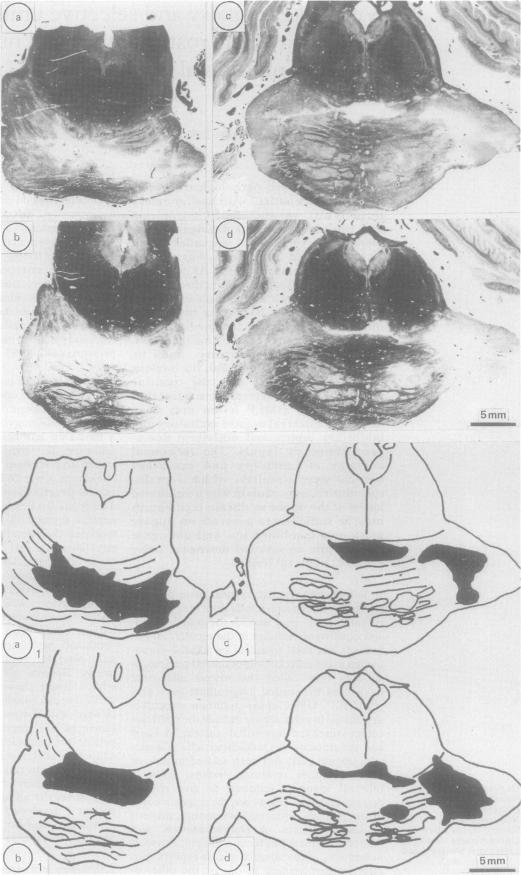
We report a clinico-pathological correlation study in a patient with basilar artery thrombosis, who developed tetraplegia and combined up- and downgaze palsy involving voluntary saccades and visually-guided movements, but sparing the oculocephalic responses. At necropsy, apart from bilateral infarction in the basis pontis, there was a single unilateral infarct selectively destroying the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF) on the right. The posterior commissure and its nucleus, the nucleus of Cajal, the nucleus of Darkschewitsch and the pontine tegmentum were spared. We suggest that the unilateral riMLF lesion may have disrupted bilateral upgaze excitatory and inhibitory inputs and unilateral downgaze excitatory inputs. The functional anatomy of inhibitory and excitatory vertical gaze circuitry, which remains speculative, may explain why a unilateral lesion of the upper midbrain tegmentum may be sufficient to generate an upgaze palsy or a combined up- and downgaze palsy, while an isolated downgaze palsy requires bilateral lesions.
我们报告了一项针对一名基底动脉血栓形成患者的临床病理相关性研究。该患者出现四肢瘫痪,并伴有向上和向下凝视麻痹,累及随意性扫视和视觉引导运动,但眼头反射保留。尸检时,除脑桥基底部双侧梗死外,右侧存在一个单一的单侧梗死灶,选择性地破坏了内侧纵束的嘴侧间质核(riMLF)。后连合及其核、 Cajal核、Darkschewitsch核和脑桥被盖部均未受累。我们认为,单侧riMLF病变可能破坏了双侧向上凝视的兴奋性和抑制性输入以及单侧向下凝视的兴奋性输入。抑制性和兴奋性垂直凝视神经回路的功能解剖学仍具有推测性,这可能解释了为什么中脑上被盖部的单侧病变可能足以导致向上凝视麻痹或向上和向下凝视联合麻痹,而孤立的向下凝视麻痹则需要双侧病变。