Division of Clinical Neurosciences, University of Edinburgh, Western General Hospital, Crewe Rd, Edinburgh EH4 2XU, UK.
BMC Neurol. 2012 Oct 18;12:123. doi: 10.1186/1471-2377-12-123.
Pyrexia after stroke (temperature ≥37.5°C) is associated with poor prognosis, but information on timing of body temperature changes and relationship to stroke severity and subtypes varies.
We recruited patients with acute ischemic stroke, measured stroke severity, stroke subtype and recorded four-hourly tympanic (body) temperature readings from admission to 120 hours after stroke. We sought causes of pyrexia and measured functional outcome at 90 days. We systematically summarised all relevant previous studies.
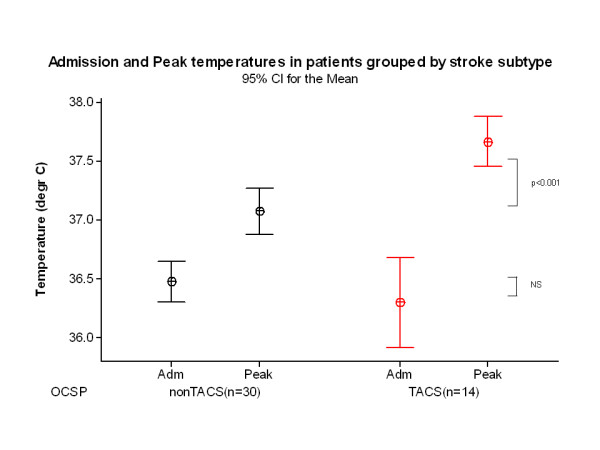
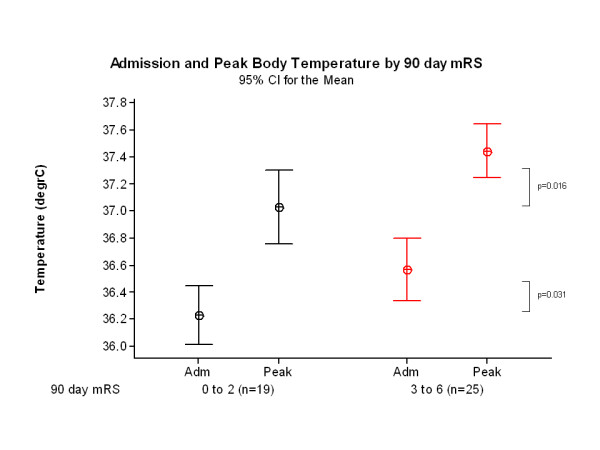
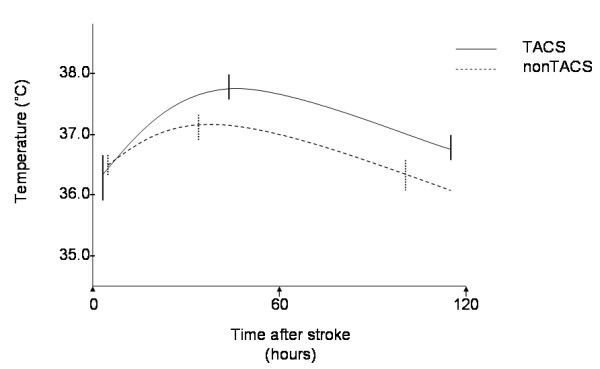
Amongst 44 patients (21 males, mean age 72 years SD 11) with median National Institute of Health Stroke Score (NIHSS) 7 (range 0-28), 14 had total anterior circulation strokes (TACS). On admission all patients, both TACS and non-TACS, were normothermic (median 36.3°C vs 36.5°C, p=0.382 respectively) at median 4 hours (interquartile range, IQR, 2-8) after stroke; admission temperature and NIHSS were not associated (r(2)=0.0, p=0.353). Peak temperature, occurring at 35.5 (IQR 19.0 to 53.8) hours after stroke, was higher in TACS (37.7°C) than non-TACS (37.1°C, p<0.001) and was associated with admission NIHSS (r(2)=0.20, p=0.002). Poor outcome (modified Rankin Scale ≥3) at 90 days was associated with higher admission (36.6°C vs. 36.2°C p=0.031) and peak (37.4°C vs. 37.0°C, p=0.016) temperatures. Sixteen (36%) patients became pyrexial, in seven (44%) of whom we found no cause other than the stroke.
Normothermia is usual within the first 4 hours of stroke. Peak temperature occurs at 1.5 to 2 days after stroke, and is related to stroke severity/subtype and more closely associated with poor outcome than admission temperature. Temperature-outcome associations after stroke are complex, but normothermia on admission should not preclude randomisation of patients into trials of therapeutic hypothermia.
卒中后发热(体温≥37.5°C)与预后不良相关,但体温变化的时间以及与卒中严重程度和亚型的关系的信息各不相同。
我们招募了急性缺血性卒中患者,测量了卒中严重程度、卒中亚型,并在卒中后 120 小时内每 4 小时记录一次鼓膜(体表)温度读数。我们寻找发热的原因,并在 90 天时测量功能结局。我们系统地总结了所有相关的既往研究。
在 44 名患者(21 名男性,平均年龄 72 岁,标准差 11)中,中位 NIHSS 评分为 7(范围 0-28),14 名患者为完全前循环梗死(TACS)。入院时,所有患者(包括 TACS 和非 TACS 患者)的体温均正常(中位 36.3°C 与 36.5°C,p=0.382),在卒中后中位 4 小时(四分位距 IQR,2-8);入院体温与 NIHSS 评分无相关性(r(2)=0.0,p=0.353)。发热峰值出现在卒中后 35.5 小时(IQR 19.0 至 53.8),TACS 患者的发热峰值(37.7°C)高于非 TACS 患者(37.1°C,p<0.001),与入院 NIHSS 评分相关(r(2)=0.20,p=0.002)。90 天时不良结局(改良 Rankin 量表≥3)与较高的入院体温(36.6°C 与 36.2°C,p=0.031)和发热峰值(37.4°C 与 37.0°C,p=0.016)相关。16 名(36%)患者出现发热,其中 7 名(44%)患者除卒中外无其他发热原因。
卒中后前 4 小时内通常体温正常。发热峰值出现在卒中后 1.5 至 2 天,与卒中严重程度/亚型相关,与入院体温相比,与不良结局的关系更密切。卒中后体温与结局的关系复杂,但入院时体温正常不应排除将患者随机分配到治疗性低温试验中。