HIV Division, Global Health Program, Bill & Melinda Gates Foundation, New Delhi, India.
PLoS One. 2012;7(11):e48827. doi: 10.1371/journal.pone.0048827. Epub 2012 Nov 15.
Evidence based resource allocation and decentralized planning of an effective HIV/AIDS response requires reliable information on levels and trends of HIV at national and sub-national geographic levels. HIV sentinel surveillance data from antenatal clinics (HSS-ANC) has been an important data source to assess the HIV/AIDS epidemic in India, but has a number of limitations. We assess the value of Prevention of Parent to Child Transmission (PPTCT) programme data to appraise the HIV epidemic in India.
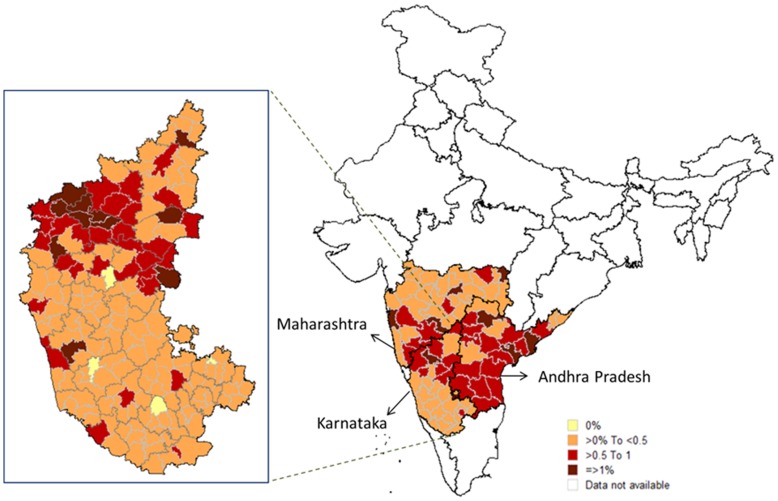
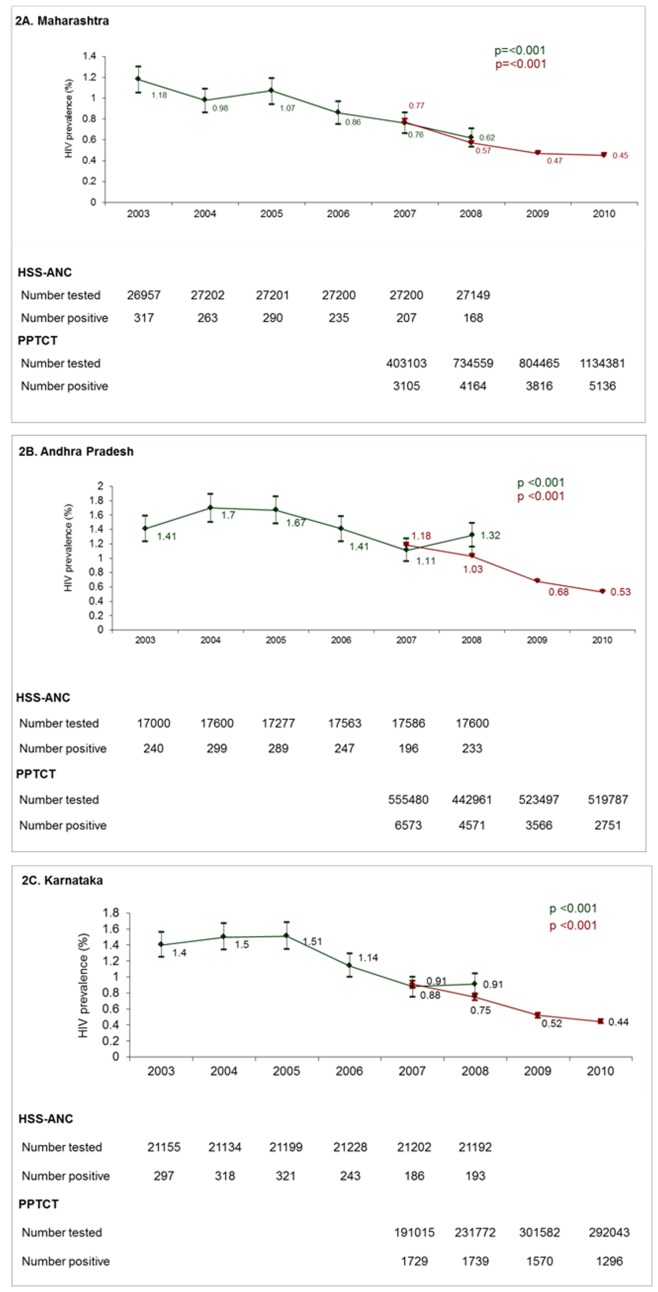
METHODS/FINDINGS: HIV data from PPTCT sites were compared to HSS-ANC and general population level surveys at various geographic levels in the states of Karnataka, Maharashtra and Andhra Pradesh. Chi-square tests were used to ascertain statistical significance. PPTCT HIV prevalence was significantly lower than HSS-ANC HIV prevalence (0.92% vs. 1.22% in Andhra Pradesh, 0.65% vs. 0.89% in Karnataka, 0.52% vs. 0.60% in Maharashtra, p<0.001 for all three states). In all three states, HIV prevalence from PPTCT centres that were part of the sentinel surveillance was comparable to HSS-ANC prevalence but significantly higher than PPTCT centres that were not part of the sentinel surveillance. HIV prevalence from PPTCT data was comparable to that from general population surveys. In all three states, significant declines in HIV prevalence between 2007 and 2010 were observed with the PPTCT data set. District level analyses of HIV trends and sub-district level analysis of HIV prevalence were possible using the PPTCT and not the HSS-ANC data sets.
HIV prevalence from PPTCT may be a better proxy for general population prevalence than HSS-ANC. PPTCT data allow for analysis of HIV prevalence and trends at smaller geographic units, which is important for decentralized planning of HIV/AIDS programming. With further improvements to the system, India could replace its HSS-ANC with PPTCT programme data for surveillance.
基于证据的资源分配和有效的艾滋病毒/艾滋病应对措施的分散规划需要有关国家和国家以下各级艾滋病毒水平和趋势的可靠信息。来自产前诊所的艾滋病毒哨点监测数据(HSS-ANC)一直是评估印度艾滋病毒/艾滋病流行情况的重要数据源,但存在许多限制。我们评估预防母婴传播(PPTCT)规划数据在评估印度艾滋病毒流行情况方面的价值。
方法/发现:将来自卡纳塔克邦、马哈拉施特拉邦和安得拉邦各州各级 HSS-ANC 和一般人群水平调查的 PPTCT 地点的艾滋病毒数据进行比较。使用卡方检验确定统计学意义。PPTCT 艾滋病毒流行率明显低于 HSS-ANC 艾滋病毒流行率(安得拉邦分别为 0.92%和 1.22%,卡纳塔克邦分别为 0.65%和 0.89%,马哈拉施特拉邦分别为 0.52%和 0.60%,所有三个州均<0.001)。在所有三个州,参与哨点监测的 PPTCT 中心的艾滋病毒流行率与 HSS-ANC 流行率相当,但明显高于未参与哨点监测的 PPTCT 中心。PPTCT 数据的艾滋病毒流行率与一般人群调查相当。在所有三个州,都观察到 2007 年至 2010 年期间 PPTCT 数据集中艾滋病毒流行率显著下降。可以使用 PPTCT 而不是 HSS-ANC 数据集进行 HIV 趋势的地区级分析和 HIV 流行率的次地区级分析。
与 HSS-ANC 相比,来自 PPTCT 的艾滋病毒流行率可能是一般人群流行率的更好替代指标。PPTCT 数据允许在更小的地理单位分析艾滋病毒流行率和趋势,这对于分散艾滋病毒/艾滋病规划的规划非常重要。随着该系统的进一步改进,印度可以用 PPTCT 规划数据代替 HSS-ANC 进行监测。