Fukino Nobutada, Oida Takatsugu, Mimatsu Kenji, Kida Kazutoshi, Kawasaki Atsushi, Kuboi Youichi, Kano Hisao
Department of Surgery, Social Insurance Yokohama Central Hospital, Yokohama, Japan.
Case Rep Gastroenterol. 2012 Sep;6(3):689-94. doi: 10.1159/000345382. Epub 2012 Nov 7.
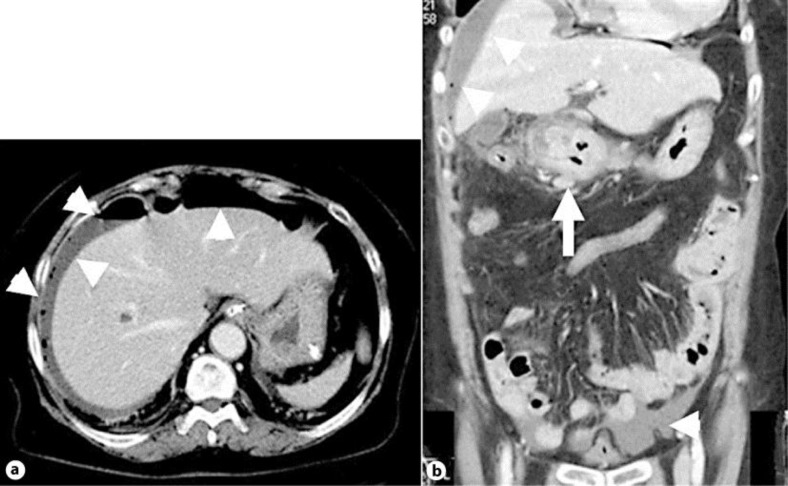
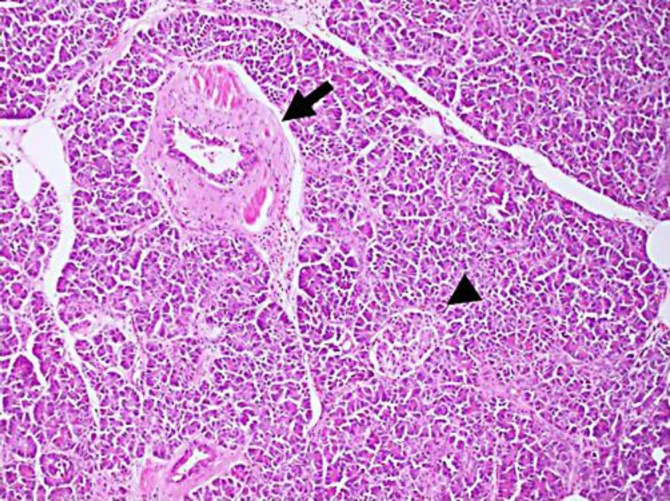
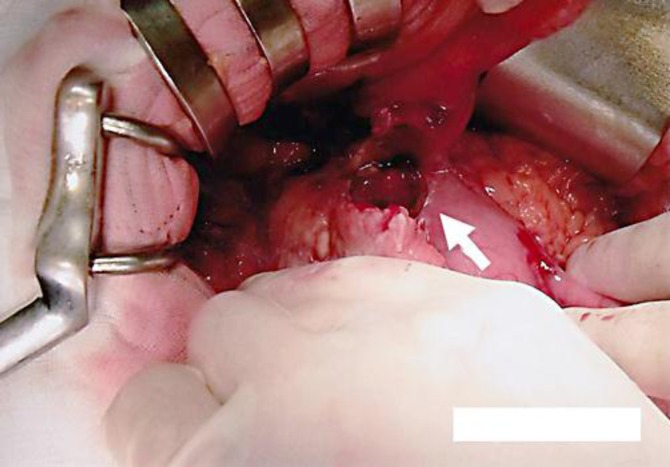
Ectopic pancreas is frequently found in the gastrointestinal tract. Lesions comprise well-developed and normally organized pancreatic tissue outside the pancreas, without anatomic or vascular connections with the true pancreas. Most patients with ectopic pancreas are asymptomatic or exhibit nonspecific symptoms. A 68-year-old Japanese woman had been experiencing intermittent pain in the right upper abdomen. Suddenly, the abdominal pain changed to intense pain in the right flank of the abdomen 2 days later. On initial medical examination, the abdomen exhibited rebound tenderness and distension. The results of laboratory tests revealed increased inflammatory reaction. Abdominal computed tomography showed free air and ascites on the surface of the liver and elevated levels of adipose tissue around the antrum and pylorus of the stomach. Perforation of the upper gastrointestinal tract was diagnosed and we performed urgent surgery. The site of perforation, whose size was 25 mm, was the lesser curvature of the antrum of the stomach. Since it was not possible to perform omentopexy, we performed extensive gastric resection. The reconstruction was a Billroth II operation. Microscopic analysis revealed pancreatic tissue within the ulceration, showing islets of Langerhans, acini, and ducts; the lesion was diagnosed as type I using Heinrich's criteria. The postoperative course was uneventful. The patient was discharged on day 13 and remains clinically healthy. Gastric perforation due to ectopic pancreas has been reported in 2 cases, including our patient, and is extremely rare. Once gastric perforation has been diagnosed, the presence of ectopic pancreas might be considered.
异位胰腺常在胃肠道中被发现。病变包括胰腺外发育良好且结构正常的胰腺组织,与真正的胰腺无解剖或血管连接。大多数异位胰腺患者无症状或表现出非特异性症状。一名68岁的日本女性右上腹一直有间歇性疼痛。两天后,腹痛突然转变为右下腹剧痛。初次体检时,腹部有反跳痛和腹胀。实验室检查结果显示炎症反应增强。腹部计算机断层扫描显示肝脏表面有游离气体和腹水,胃窦和幽门周围脂肪组织水平升高。诊断为上消化道穿孔,我们进行了紧急手术。穿孔部位在胃窦小弯处,大小为25毫米。由于无法进行网膜固定术,我们进行了广泛的胃切除术。重建采用毕罗Ⅱ式手术。显微镜分析显示溃疡内有胰腺组织,可见胰岛、腺泡和导管;根据海因里希标准,该病变被诊断为Ⅰ型。术后过程顺利。患者于第13天出院,目前临床状况良好。包括我们的患者在内,已有2例报道异位胰腺导致胃穿孔,极为罕见。一旦诊断为胃穿孔,可能需要考虑异位胰腺的存在。