Discipline of Oral & Maxillofacial Surgery, Faculty of Dentistry, The University of Hong Kong, Hong Kong, Hong Kong SAR.
PLoS One. 2012;7(11):e49585. doi: 10.1371/journal.pone.0049585. Epub 2012 Nov 19.
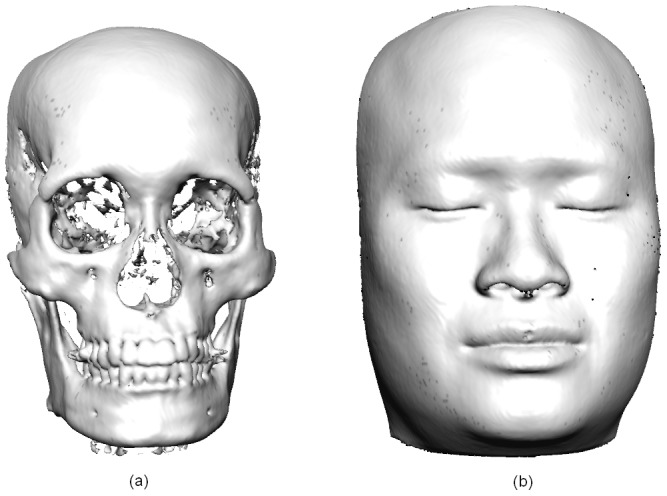
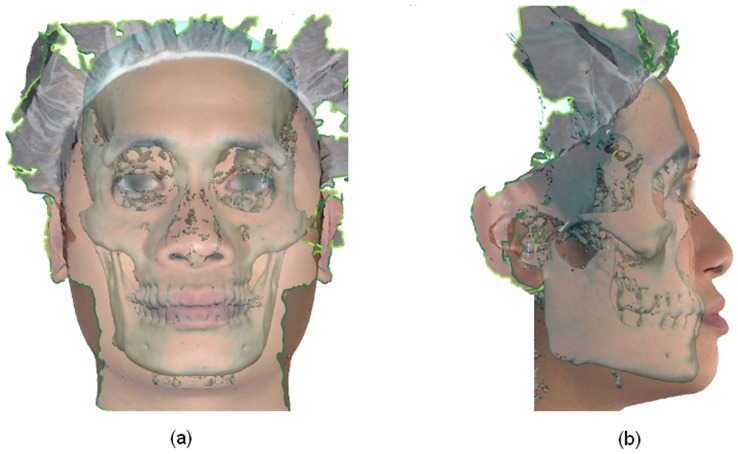
Cone-beam Computed Tomography (CBCT) and stereophotography are two of the latest imaging modalities available for three-dimensional (3-D) visualization of craniofacial structures. However, CBCT provides only limited information on surface texture. This can be overcome by combining the bone images derived from CBCT with 3-D photographs. The objectives of this study were 1) to evaluate the feasibility of integrating 3-D Photos and CBCT images 2) to assess degree of error that may occur during the above processes and 3) to identify facial regions that would be most appropriate for 3-D image registration.
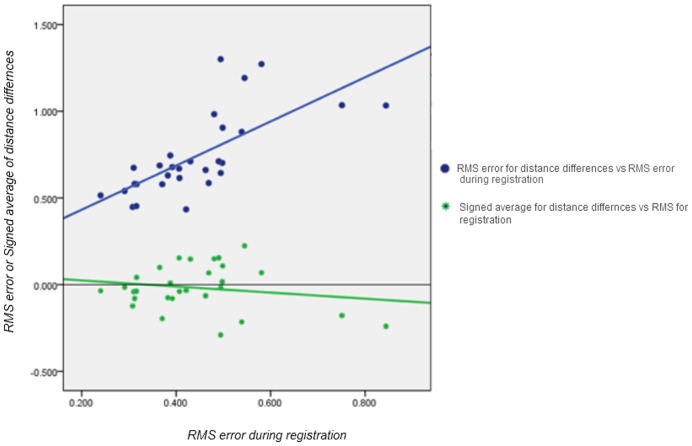
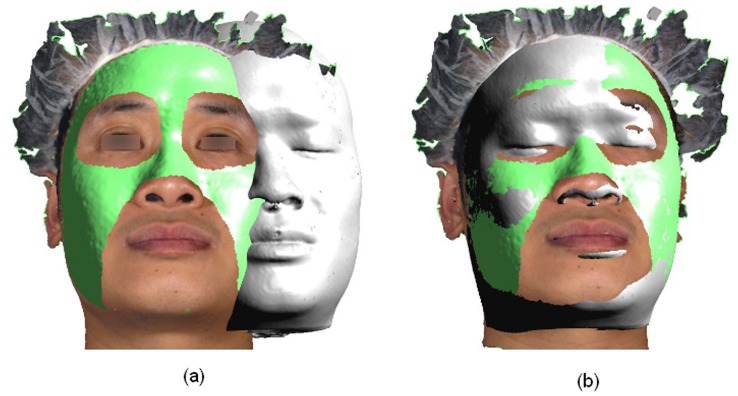
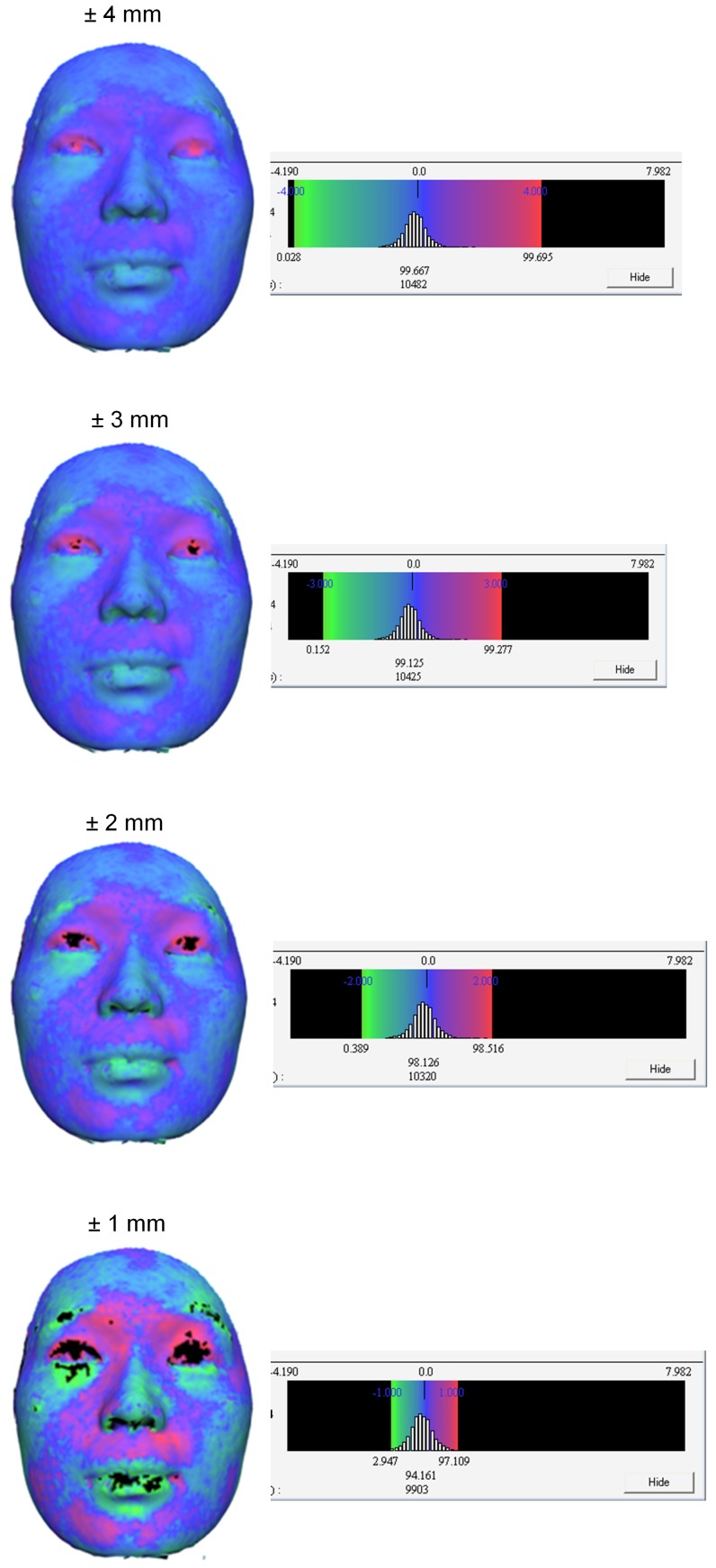
CBCT scans and stereophotographic images from 29 patients were used for this study. Two 3-D images corresponding to the skin and bone were extracted from the CBCT data. The 3-D photo was superimposed on the CBCT skin image using relatively immobile areas of the face as a reference. 3-D colour maps were used to assess the accuracy of superimposition were distance differences between the CBCT and 3-D photo were recorded as the signed average and the Root Mean Square (RMS) error.
The signed average and RMS of the distance differences between the registered surfaces were -0.018 (±0.129) mm and 0.739 (±0.239) mm respectively. The most errors were found in areas surrounding the lips and the eyes, while minimal errors were noted in the forehead, root of the nose and zygoma.
CBCT and 3-D photographic data can be successfully fused with minimal errors. When compared to RMS, the signed average was found to under-represent the registration error. The virtual 3-D composite craniofacial models permit concurrent assessment of bone and soft tissues during diagnosis and treatment planning.
锥形束 CT(CBCT)和立体摄影术是两种最新的成像方式,可用于三维(3-D)颅面结构可视化。然而,CBCT 仅提供关于表面纹理的有限信息。通过将源自 CBCT 的骨图像与 3-D 照片相结合,可以克服这一问题。本研究的目的是:1)评估整合 3-D 照片和 CBCT 图像的可行性;2)评估上述过程中可能出现的误差程度;3)确定最适合 3-D 图像配准的面部区域。
本研究使用了 29 名患者的 CBCT 扫描和立体摄影图像。从 CBCT 数据中提取出两个对应皮肤和骨骼的 3-D 图像。使用面部相对固定的区域作为参考,将 3-D 照片叠加到 CBCT 皮肤图像上。使用 3-D 彩色地图评估叠加的准确性,并记录 CBCT 和 3-D 照片之间的距离差异作为有符号平均值和均方根(RMS)误差。
注册表面之间的距离差异的有符号平均值和 RMS 分别为-0.018(±0.129)mm 和 0.739(±0.239)mm。误差最大的区域是嘴唇和眼睛周围,而额头、鼻子根部和颧骨区域的误差最小。
可以成功地融合 CBCT 和 3-D 摄影数据,误差最小。与 RMS 相比,有符号平均值被发现低估了配准误差。虚拟 3-D 复合颅面模型允许在诊断和治疗计划期间同时评估骨骼和软组织。