Park Nicollet Institute, Minneapolis, MN, USA.
Osteoporos Int. 2013 Mar;24(3):801-10. doi: 10.1007/s00198-012-2210-8. Epub 2012 Dec 4.
In the Study of Osteoporotic Fractures (SOF), 18.5 % of incident hip fractures identified in Medicare Fee-for-Service claims data were not reported to or confirmed by the cohort. Cognitive impairment was a modest risk factor for false-negative hip fracture ascertainment via self-report.
Prospective cohort studies of fractures that rely on participant self-report to be the initial signal of an incident fracture could be prone to bias if a significant proportion of fractures are not self-reported.
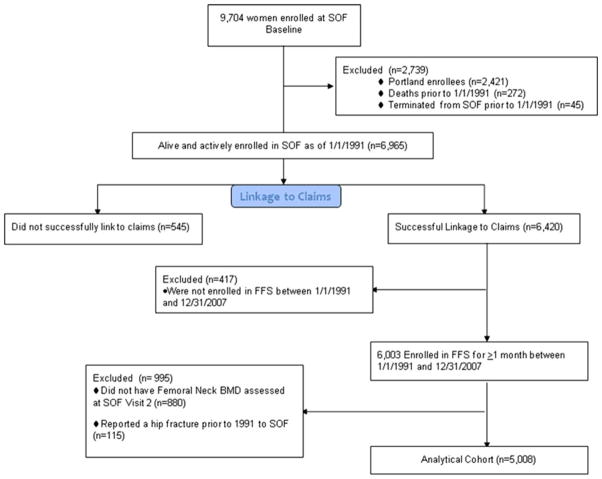
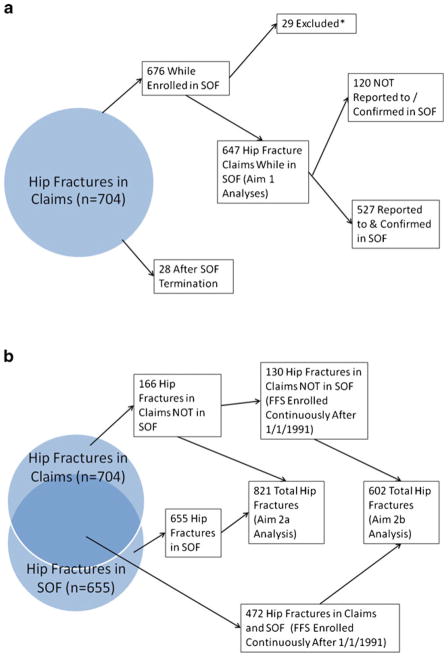
We used data from the SOF merged with Medicare Fee-for-Service claims data to estimate the proportion of participants who had an incident hip fracture identified in Medicare claims that was either not self-reported or confirmed (by review of radiographic reports) in SOF.
Between 1/1/1991 and 12/31/2007, 647 SOF participants had a hip fracture identified in Medicare claims, but 120 (18.5 %) were either not reported to or confirmed by the cohort. False-negative hip fracture ascertainment was associated with a reduced modified Mini-Mental State Exam (MMSE) score (odds ratio 1.31 per SD decrease, 95 % C.I. 1.06-1.63). Point estimates of associations of predictors of incident hip fracture were changed minimally when the misclassification of incident hip fracture status was corrected with use of claims data.
A substantial minority of incident hip fractures were not reported to or confirmed in the SOF. Cognitive impairment was modestly associated with false-negative hip fracture ascertainment. While there was no evidence to suggest that misclassification of incident hip fracture status resulted in biased associations of potential predictors with hip fracture in this study, false-negative incident fracture ascertainment in smaller cohort studies with limited power may increase the risk of type 2 error (not finding significant associations of predictors with incident fractures).
在骨质疏松性骨折研究(SOF)中,在医疗保险按服务收费数据中发现的 18.5%的新发髋部骨折未向队列报告或经队列确认。认知障碍是通过自我报告进行假阴性髋部骨折确定的适度危险因素。
依赖参与者自我报告作为新发骨折初始信号的骨折前瞻性队列研究,如果有相当比例的骨折未被自我报告,可能容易出现偏倚。
我们使用来自 SOF 的数据与医疗保险按服务收费数据合并,以估计在医疗保险索赔中确定的、但在 SOF 中既未报告也未经确认(通过审查放射报告)的参与者新发髋部骨折的比例。
在 1991 年 1 月 1 日至 2007 年 12 月 31 日期间,647 名 SOF 参与者的髋部骨折在医疗保险索赔中得到确认,但有 120 名(18.5%)既未向队列报告也未经队列确认。假阴性髋部骨折确定与改良的 Mini-Mental State 检查(MMSE)评分降低相关(每标准差降低的比值比为 1.31,95%置信区间为 1.06-1.63)。当使用索赔数据纠正新发髋部骨折状态的分类错误时,与新发髋部骨折相关的预测因子的点估计关联变化很小。
相当一部分新发髋部骨折未向 SOF 报告或确认。认知障碍与假阴性髋部骨折确定适度相关。虽然没有证据表明,在这项研究中,新发髋部骨折状态的分类错误导致潜在预测因子与髋部骨折的关联存在偏倚,但在样本量较小且能力有限的队列研究中,假阴性的新发骨折确定可能会增加 2 型错误(未发现预测因子与新发骨折的显著关联)的风险。