Department of Cardiology, Oakwood Hospital and Medical Center, Dearborn, Michigan, USA.
Diabetes Care. 2013 Apr;36(4):972-7. doi: 10.2337/dc12-1548. Epub 2012 Dec 10.
In type 2 diabetes mellitus (T2DM), it remains unclear whether coronary artery calcium (CAC) provides additional information about cardiovascular disease (CVD) mortality beyond the Framingham Risk Score (FRS) factors.
A total of 1,123 T2DM participants, ages 34-86 years, in the Diabetes Heart Study followed up for an average of 7.4 years were separated using baseline computed tomography scans of CAC (0-9, 10-99, 100-299, 300-999, and ≥1,000). Logistic regression was performed to examine the association between CAC and CVD mortality adjusting for FRS. Areas under the curve (AUC) with and without CAC were compared. Net reclassification improvement (NRI) compared FRS (model 1) versus FRS+CAC (model 2) using 7.4-year CVD mortality risk categories 0% to <7%, 7% to <20%, and ≥20%.
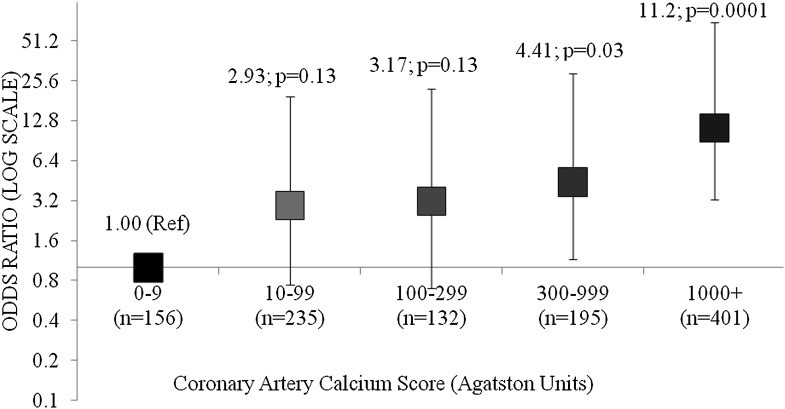
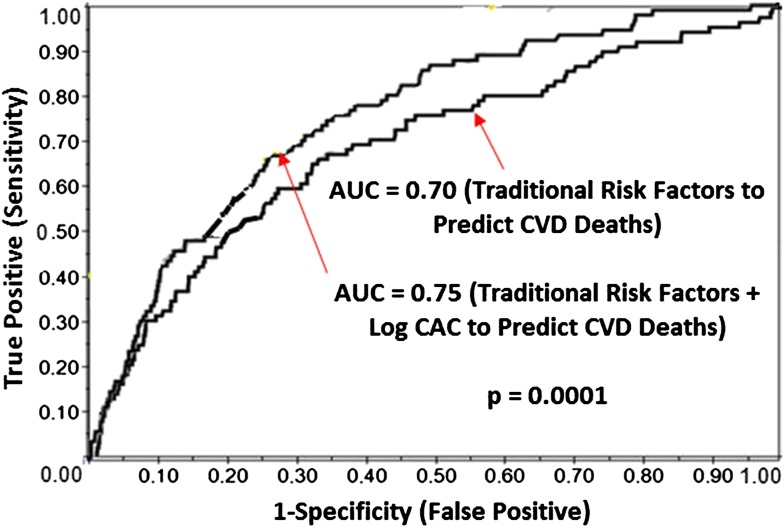
Overall, 8% of participants died of cardiovascular causes during follow-up. In multivariate analysis, the odds ratios (95% CI) for CVD mortality using CAC 0-9 as the reference group were, CAC 10-99: 2.93 (0.74-19.55); CAC 100-299: 3.17 (0.70-22.22); CAC 300-999: 4.41(1.15-29.00); and CAC ≥1,000: 11.23 (3.24-71.00). AUC (95% CI) without CAC was 0.70 (0.67-0.73), AUC with CAC was 0.75 (0.72-0.78), and NRI was 0.13 (0.07-0.19).
In T2DM, CAC predicts CVD mortality and meaningfully reclassifies participants, suggesting clinical utility as a risk stratification tool in a population already at increased CVD risk.
在 2 型糖尿病(T2DM)患者中,冠状动脉钙(CAC)评分是否能提供Framingham 风险评分(FRS)以外的心血管疾病(CVD)死亡率的额外信息仍不清楚。
共有 1123 名年龄在 34-86 岁的 T2DM 患者参加了糖尿病心脏研究,平均随访 7.4 年,基线时使用 CAC 的计算机断层扫描(0-9、10-99、100-299、300-999 和≥1000)对其进行分组。使用逻辑回归分析 CAC 与 CVD 死亡率之间的关系,并在调整 FRS 后进行分析。比较有无 CAC 时的曲线下面积(AUC)。使用 7.4 年 CVD 死亡率风险类别(0%-<7%、7%-<20%和≥20%),比较 FRS(模型 1)与 FRS+CAC(模型 2)的净重新分类改善(NRI)。
总体而言,8%的参与者在随访期间死于心血管原因。在多变量分析中,以 CAC 0-9 为参考组,CAC 10-99、CAC 100-299、CAC 300-999 和 CAC≥1000 的 CVD 死亡率比值比(95%CI)分别为 2.93(0.74-19.55)、3.17(0.70-22.22)、4.41(1.15-29.00)和 11.23(3.24-71.00)。无 CAC 时的 AUC(95%CI)为 0.70(0.67-0.73),有 CAC 时的 AUC 为 0.75(0.72-0.78),NRI 为 0.13(0.07-0.19)。
在 T2DM 患者中,CAC 预测 CVD 死亡率,并对患者进行有意义的重新分类,提示 CAC 作为一种风险分层工具具有临床应用价值,尤其适用于已经处于 CVD 风险增加的人群。