Guerra Carmen, Linde-Zwirble Walter T, Wunsch Hannah
Crit Care. 2012 Dec 17;16(6):R233. doi: 10.1186/cc11901.
Hospitalization increases the risk of a subsequent diagnosis of dementia. We aimed to identify diagnoses or events during a hospitalization requiring critical care that are associated with a subsequent dementia diagnosis in the elderly.
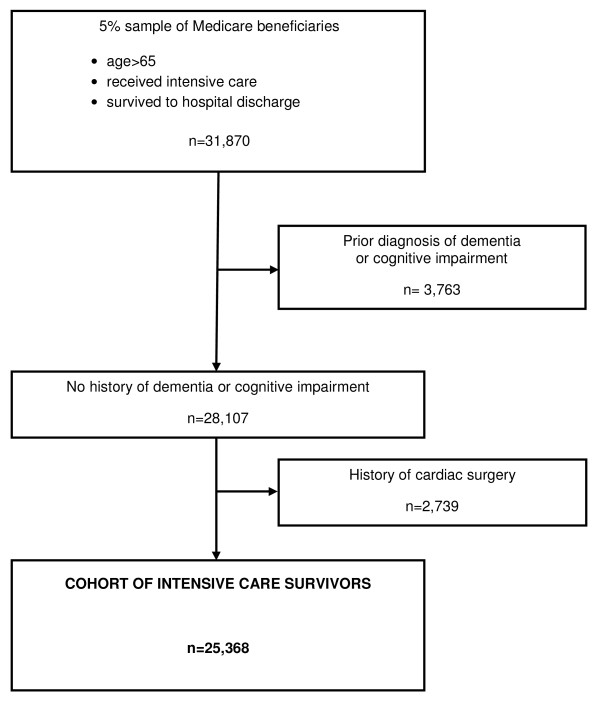
A cohort study of a random 5% sample of Medicare beneficiaries who received intensive care in 2005 and survived to hospital discharge, with three years of follow-up (through 2008) was conducted using Medicare claims files. We defined dementia using the International Classification of Diseases, 9th edition, clinical modification (ICD-9-CM) codes and excluded patients with any prior diagnosis of dementia or cognitive impairment in the year prior to admission. We used an extended Cox model to examine the association between diagnoses and events associated with the critical illness and a subsequent diagnosis of dementia, adjusting for known risk factors for dementia.
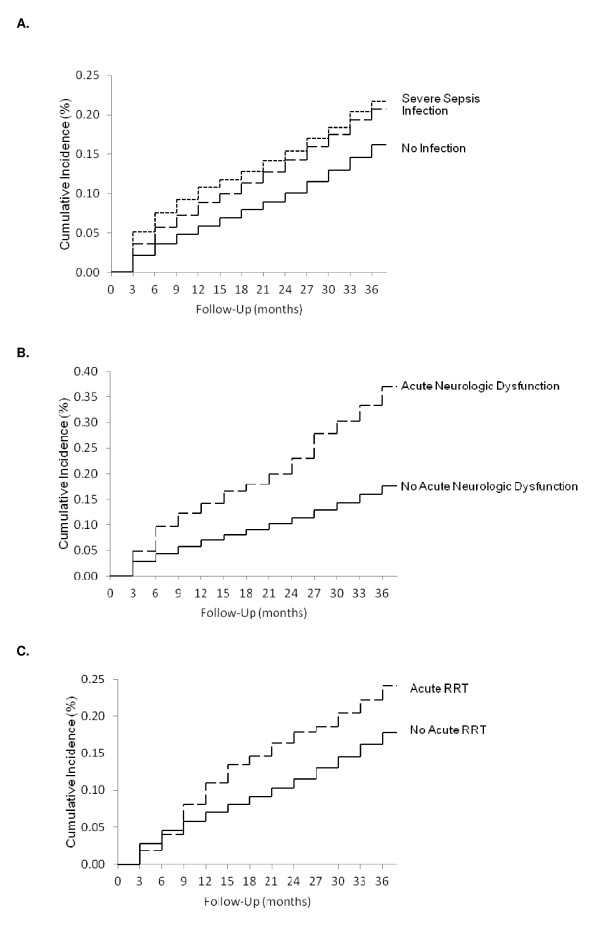
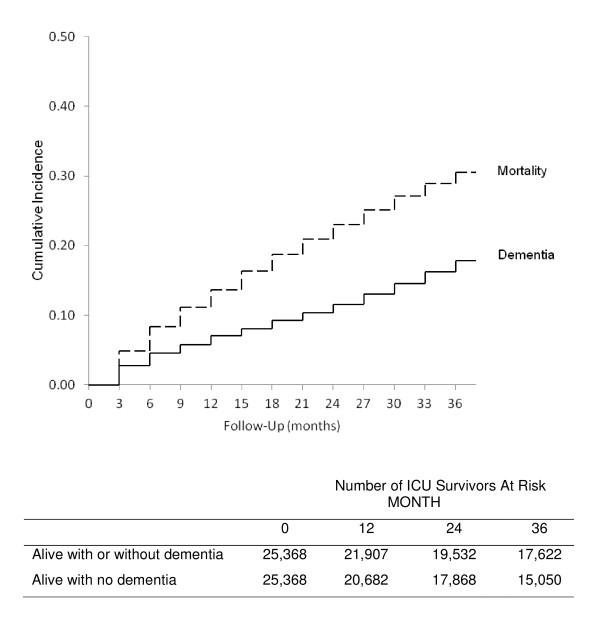
Over the three years of follow-up, dementia was newly diagnosed in 4,519 (17.8%) of 25,368 patients who received intensive care and survived to hospital discharge. After accounting for known risk factors, having an infection (adjusted hazard ratio (AHR) = 1.25; 95% CI, 1.17 to 1.35), or a diagnosis of severe sepsis (AHR = 1.40; 95% CI, 1.28 to 1.53), acute neurologic dysfunction (AHR = 2.06; 95% CI, 1.72 to 2.46), and acute dialysis (AHR = 1.70; 95% CI, 1.30 to 2.23) were all independently associated with a subsequent diagnosis of dementia. No other measured ICU factors, such as need for mechanical ventilation, were independently associated.
Among ICU events, infection or severe sepsis, neurologic dysfunction, and acute dialysis were independently associated with a subsequent diagnosis of dementia. Patient prognostication, as well as future research into post-ICU cognitive decline, should focus on these higher-risk subgroups.
住院会增加随后被诊断为痴呆症的风险。我们旨在确定在需要重症监护的住院期间与老年患者随后的痴呆症诊断相关的诊断或事件。
利用医疗保险理赔档案对2005年接受重症监护并存活至出院的5%医疗保险受益人的随机样本进行队列研究,并进行三年随访(至2008年)。我们使用国际疾病分类第九版临床修订本(ICD-9-CM)编码定义痴呆症,并排除入院前一年有任何痴呆症或认知障碍既往诊断的患者。我们使用扩展的Cox模型来检验与危重病相关的诊断和事件与随后的痴呆症诊断之间的关联,并对已知的痴呆症风险因素进行调整。
在三年随访期间,25368名接受重症监护并存活至出院的患者中有4519名(17.8%)被新诊断为痴呆症。在考虑已知风险因素后,发生感染(调整后风险比[AHR]=1.25;95%置信区间,1.17至1.35)、诊断为严重脓毒症(AHR=1.40;95%置信区间,1.28至1.53)、急性神经功能障碍(AHR=2.06;95%置信区间,1.72至2.46)和急性透析(AHR=1.70;95%置信区间,1.30至2.23)均与随后的痴呆症诊断独立相关。没有其他测量的重症监护病房因素,如机械通气需求,与之独立相关。
在重症监护病房事件中,感染或严重脓毒症、神经功能障碍和急性透析与随后的痴呆症诊断独立相关。患者预后以及未来对重症监护病房后认知功能下降的研究应关注这些高危亚组。