SurgOne P.C., Swedish Medical Center, 401 W Hampden Place Suite 230, Englewood, CO 80110, USA.
Surg Endosc. 2013 Jun;27(6):1997-2004. doi: 10.1007/s00464-012-2700-y. Epub 2013 Jan 9.
Hiatal repair failure is the nemesis of laparoscopic paraesophageal hernia repair as well as the major cause of failure of primary fundoplication and reoperation on the hiatus. Biologic prosthetics offer the promise of reinforcing the repair without risks associated with permanent prosthetics.
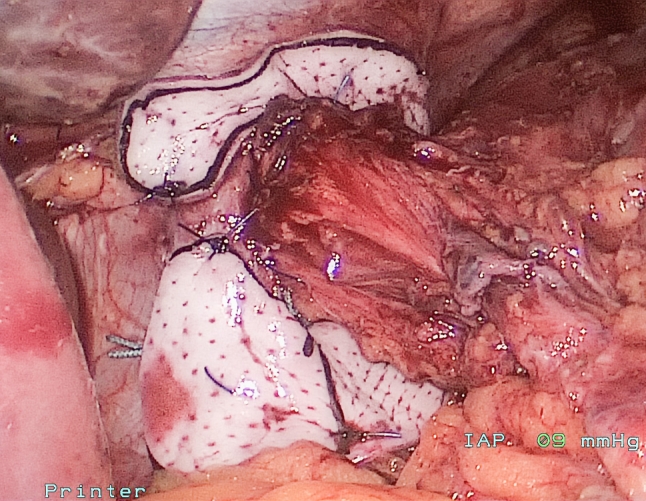
Retrospective evaluation of safety and relative efficacy of laparoscopic hiatal hernia repair using an allograft (acellular dermal matrix) onlay. Patients with symptomatic failures underwent endoscopic or radiographic assessment of hiatal status.
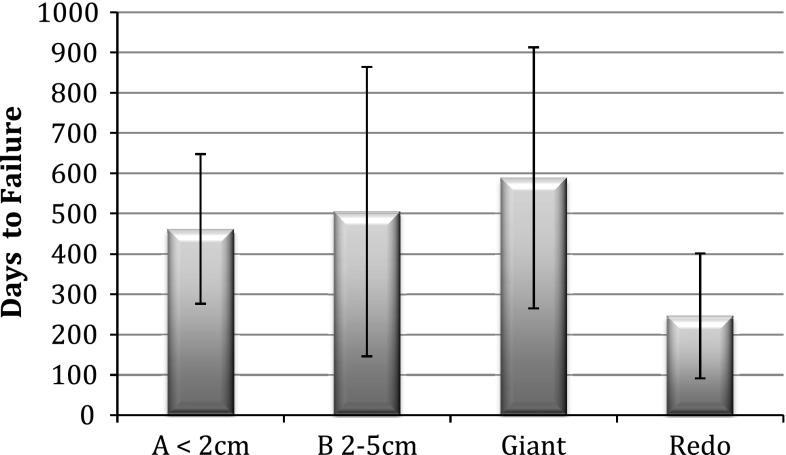
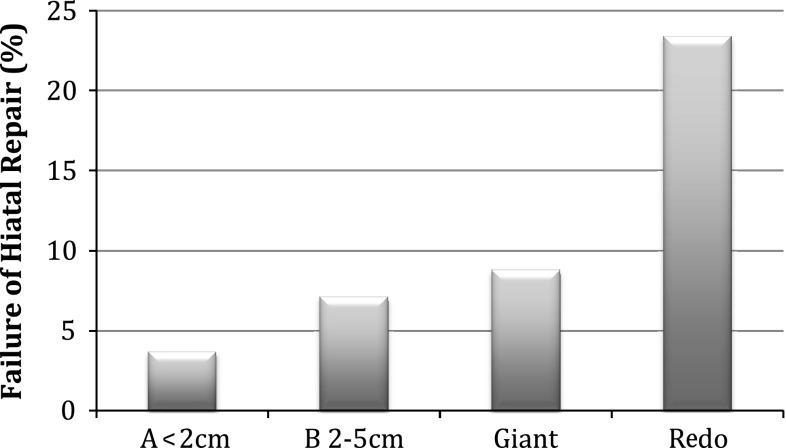
Greater than 6-month follow-up was available for 252 of 450 consecutive patients undergoing laparoscopic allograft-reinforced hiatal hernia repair between January 2007 and March 2011. No erosions, strictures, or persisting dysphagia were encountered. Adhesions were minimal in cases where reoperation was required. Failure of the hiatal repair at median 18 months (6-51 months) was significantly (p < 0.005) different between groups: group A (primary fundoplication with axial hernia ≤ 2 cm), 3.7 %; group B (primary fundoplication with axial hernia 2-5 cm), 7.1 %; group G (giant/paraesophageal), 8.8 %; group R (reoperative), 23.4 %. Additionally, mean time to failure was significantly shorter in group R (247 days) compared with the other groups (462-489 days).
Use of allograft reinforcement to the hiatus is safe at 18 months median follow-up. Reoperations had a significantly higher failure rate and shorter time to failure than the other groups despite allograft, suggesting that primary repairs require utmost attention and that additional techniques may be needed in reoperations. Patients with hiatal hernias >2 cm axially had a recurrence rate equal to that of patients undergoing paraesophageal hiatal hernia repair, and should be treated similarly.
食管裂孔疝修补术后失败是腹腔镜食管裂孔疝修补术的噩梦,也是原发性胃底折叠术失败和裂孔再手术的主要原因。生物假体提供了加强修复的可能性,而没有与永久性假体相关的风险。
回顾性评估使用同种异体(脱细胞真皮基质)补片的腹腔镜食管裂孔疝修补术的安全性和相对疗效。有症状失败的患者接受内镜或影像学评估裂孔状态。
2007 年 1 月至 2011 年 3 月期间,连续 450 例接受腹腔镜同种异体增强食管裂孔疝修补术的患者中,有 252 例获得了超过 6 个月的随访。未发现穿孔、狭窄或持续吞咽困难。需要再次手术的病例中粘连很少。中位 18 个月(6-51 个月)时食管裂孔修复失败的发生率在各组之间差异显著(p<0.005):A 组(原发性胃底折叠术伴轴向疝≤2cm)为 3.7%;B 组(原发性胃底折叠术伴轴向疝 2-5cm)为 7.1%;G 组(巨大/食管裂孔旁疝)为 8.8%;R 组(再次手术)为 23.4%。此外,R 组(247 天)的平均失败时间明显短于其他组(462-489 天)。
在中位随访 18 个月时,使用同种异体补片增强裂孔是安全的。尽管使用了同种异体补片,但再手术组的失败率和失败时间明显更高,这表明原发性修复需要格外注意,并且可能需要额外的技术,对于轴向疝径>2cm 的食管裂孔疝患者,其复发率与行食管裂孔旁疝修补术的患者相同,应采用类似的治疗方法。