Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden.
PLoS One. 2012;7(12):e51420. doi: 10.1371/journal.pone.0051420. Epub 2012 Dec 27.
In order to achieve Millennium Development Goals 4, 5 and 6, it is essential to address adolescents' health.
To estimate the additional resources required to scale up adolescent friendly health service interventions with the objective to reduce mortality and morbidity among individuals aged 10 to 19 years in 74 low- and middle- income countries.
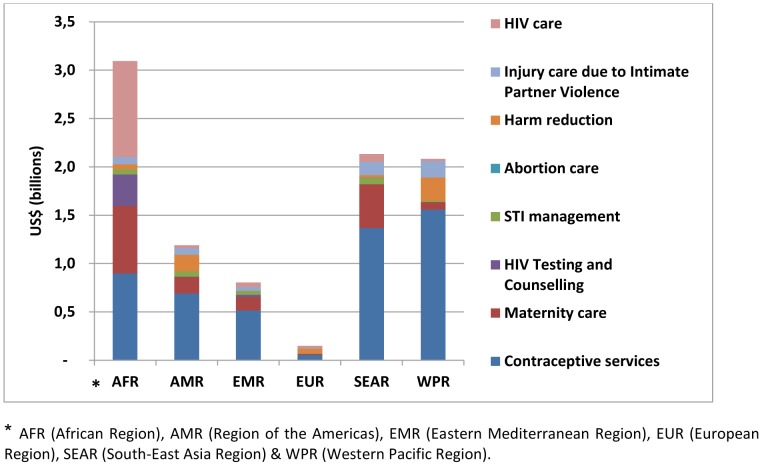
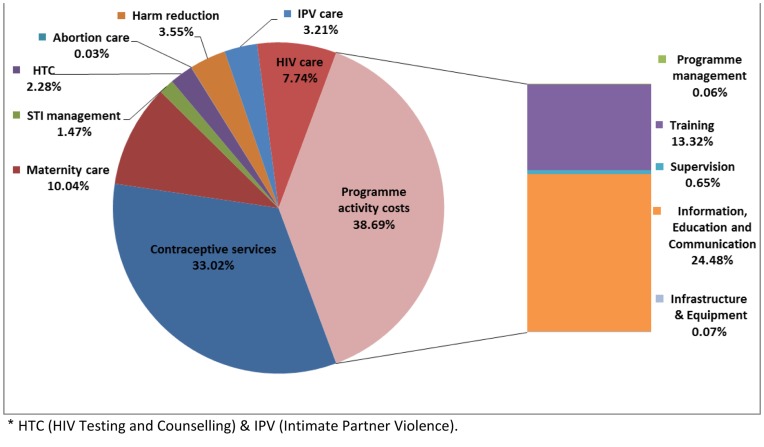
A costing model was developed to estimate the financial resources needed to scale-up delivery of a set of interventions including contraception, maternity care, management of sexually transmitted infections, HIV testing and counseling, safe abortion services, HIV harm reduction, HIV care and treatment and care of injuries due to intimate partner physical and sexual violence. Financial costs were estimated for each intervention, country and year using a bottom-up ingredients approach, defining costs at different levels of delivery (i.e., community, health centre, and hospital level). Programme activity costs to improve quality of care were also estimated, including activities undertaken at national-, district- and facility level in order to improve adolescents' use of health services (i.e., to render health services adolescent friendly).
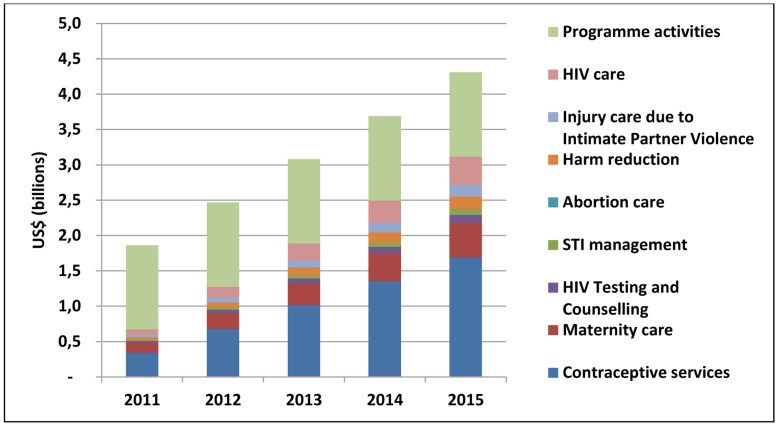
Costs of achieving universal coverage are estimated at an additional US$ 15.41 billion for the period 2011-2015, increasing from US$ 1.86 billion in 2011 to US$ 4,31 billion in 2015. This corresponds to approximately US$ 1.02 per adolescent in 2011, increasing to 4.70 in 2015. On average, for all 74 countries, an annual additional expenditure per capita ranging from of US$ 0.38 in 2011 to US$ 0.82 in 2015, would be required to support the scale-up of key adolescent friendly health services.
The estimated costs show a substantial investment gap and are indicative of the additional investments required to scale up health service delivery to adolescents towards universal coverage by 2015.
为了实现千年发展目标 4、5 和 6,解决青少年健康问题至关重要。
评估扩大青少年友好型卫生服务干预措施所需的额外资源,以降低 74 个中低收入国家 10 至 19 岁人群的死亡率和发病率。
开发了一个成本模型来估算扩大一系列干预措施所需的财政资源,这些干预措施包括避孕、产妇保健、性传播感染管理、艾滋病毒检测和咨询、安全堕胎服务、艾滋病毒减少危害、艾滋病毒护理和治疗以及因亲密伴侣身体和性暴力而导致的伤害护理。使用自下而上的成分方法估算了每个干预措施、国家和年份的财务成本,将成本定义为不同交付水平(即社区、卫生中心和医院)的成本。还估算了改善护理质量的方案活动成本,包括在国家、地区和设施各级开展的活动,以提高青少年对卫生服务的利用(即使卫生服务对青少年友好)。
2011 年至 2015 年期间,实现普及覆盖的成本估计增加 154.1 亿美元,从 2011 年的 18.6 亿美元增加到 2015 年的 431 亿美元。这相当于 2011 年每个青少年约 1.02 美元,到 2015 年增加到 4.70 美元。平均而言,对于所有 74 个国家,在 2011 年至 2015 年期间,每年需要增加人均额外支出,范围从 0.38 美元增加到 0.82 美元,以支持扩大青少年友好型卫生服务。
估计成本显示出巨大的投资差距,表明需要额外投资以扩大 2015 年之前向青少年普及卫生服务的提供。