Ginzburg Serge, Nevers Thomas, Staff Ilene, Tortora Joseph, Champagne Alison, Kesler Stuart S, Laudone Vincent P, Wagner Joseph R
University of Connecticut Health Center, Farmington, CT, USA.
JSLS. 2012 Jul-Sep;16(3):443-50. doi: 10.4293/108680812X13462882736538.
To determine prostate cancer biochemical recurrence rates with respect to surgical margin (SM) status for patients undergoing robotic-assisted laparoscopic radical prostatectomy (RALP).
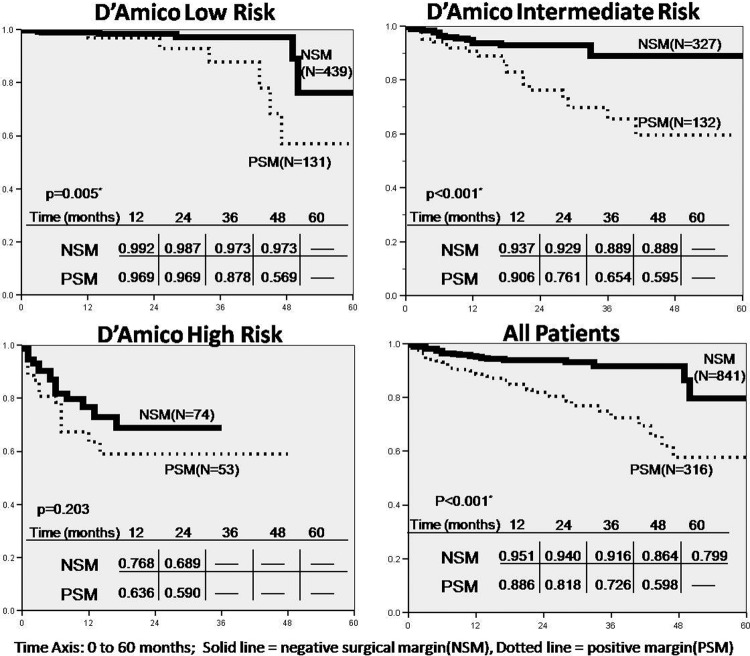
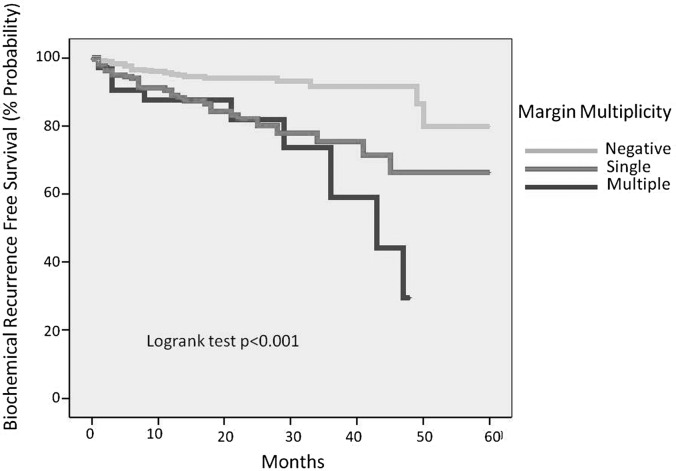
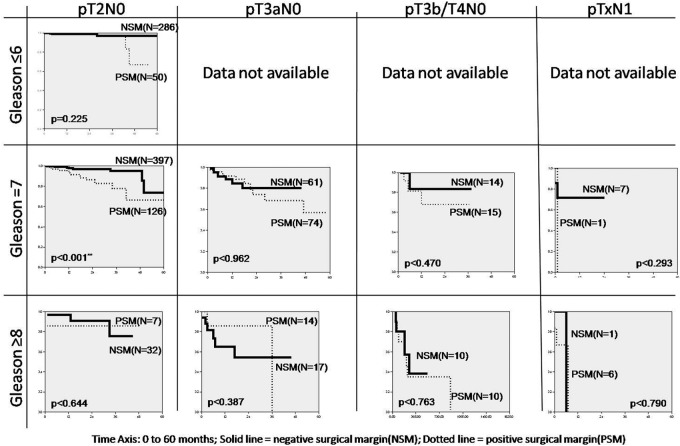
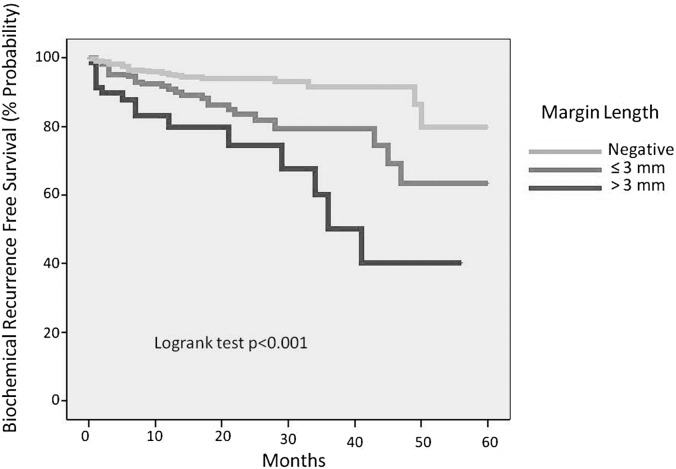
IRB-approved radical prostatectomy database was queried. Patients were stratified as low, intermediate, and high risk according to D'Amico's risk classification. Postoperative prostate-specific antigen (PSA) values were obtained every 3 mo for the first year, then biannually and annually thereafter. Biochemical recurrence was defined as ≥0.2ng/mL. Patients receiving adjuvant or salvage treatment were included. Positive surgical margin was defined as presence of cancer cells at inked resection margin in the final specimen. Margin presence (negative/positive), margin multiplicity (single/multiple), and margin length (≤ 3mm focal and >3mm extensive) were noted. Kaplan-Meier curves of biochemical recurrence-free survival (BRFS) as a function of SM were generated. Forward stepwise multivariate Cox regression was performed, with preoperative PSA, Gleason score, pathologic stage, prostate gland weight, and SM as covariates.
At our institution, 1437 patients underwent RALP (2003-2009). Of these, 1159 had sufficient data and were included in our analysis. Mean follow-up was 16 mo. Kaplan-Meier curves demonstrated significant increase in BRFS in low-risk and intermediate-risk groups with negative SM. Overall BRFS at 5 y was 72%. Gleason score, pathologic stage, and SM status were significant prognostic factors in multivariate analysis.
Negative surgical margins resulted in lower biochemical recurrence rates for low-risk and intermediate-risk groups. Multifocal and longer positive margins were associated with higher biochemical recurrence rates compared with unifocal and shorter positive margins. Documenting biochemical recurrence rates for RALP is important, because this treatment for localized prostate cancer is validated.
确定接受机器人辅助腹腔镜根治性前列腺切除术(RALP)的患者前列腺癌生化复发率与手术切缘(SM)状态的关系。
查询经机构审查委员会批准的根治性前列腺切除术数据库。根据达米科风险分类将患者分为低、中、高风险组。术后第一年每3个月获取前列腺特异性抗原(PSA)值,此后每半年和每年获取一次。生化复发定义为PSA≥0.2ng/mL。纳入接受辅助或挽救性治疗的患者。阳性手术切缘定义为最终标本中墨染切除边缘存在癌细胞。记录切缘情况(阴性/阳性)、切缘数量(单个/多个)和切缘长度(≤3mm局灶性和>3mm广泛性)。生成以SM为函数的生化无复发生存(BRFS)的Kaplan-Meier曲线。进行向前逐步多变量Cox回归分析,将术前PSA、Gleason评分、病理分期、前列腺重量和SM作为协变量。
在我们机构,1437例患者接受了RALP(2003 - 2009年)。其中,1159例有足够数据并纳入我们的分析。平均随访时间为16个月。Kaplan-Meier曲线显示,低风险和中风险组中SM阴性的患者BRFS显著增加。5年时总体BRFS为72%。在多变量分析中,Gleason评分、病理分期和SM状态是显著的预后因素。
阴性手术切缘导致低风险和中风险组的生化复发率较低。与单灶性和较短的阳性切缘相比,多灶性和较长的阳性切缘与较高的生化复发率相关。记录RALP的生化复发率很重要,因为这种治疗局限性前列腺癌的方法已得到验证。