NYU School of Medicine, New York, NY 10016, USA.
J Clin Rheumatol. 2013 Jan;19(1):19-29. doi: 10.1097/RHU.0b013e31827d8790.
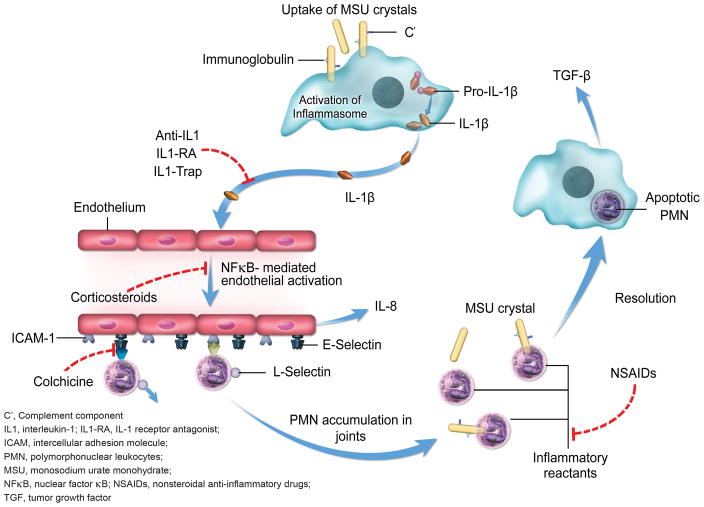
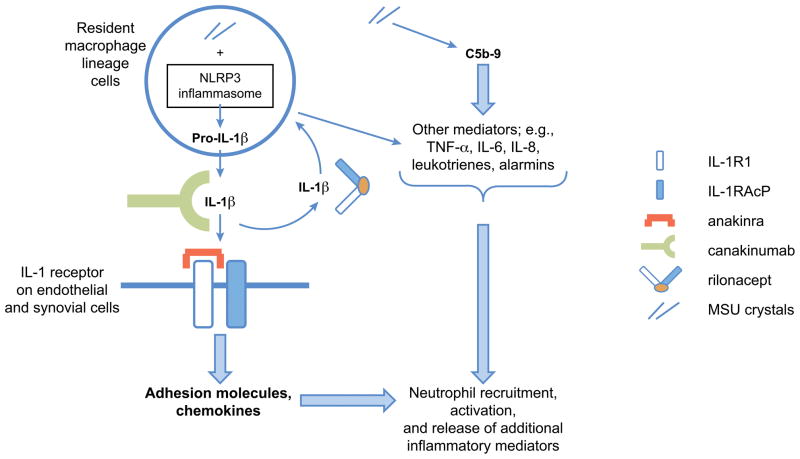
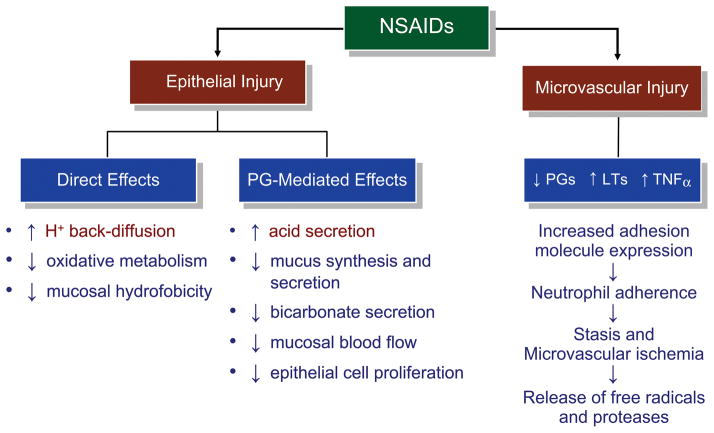
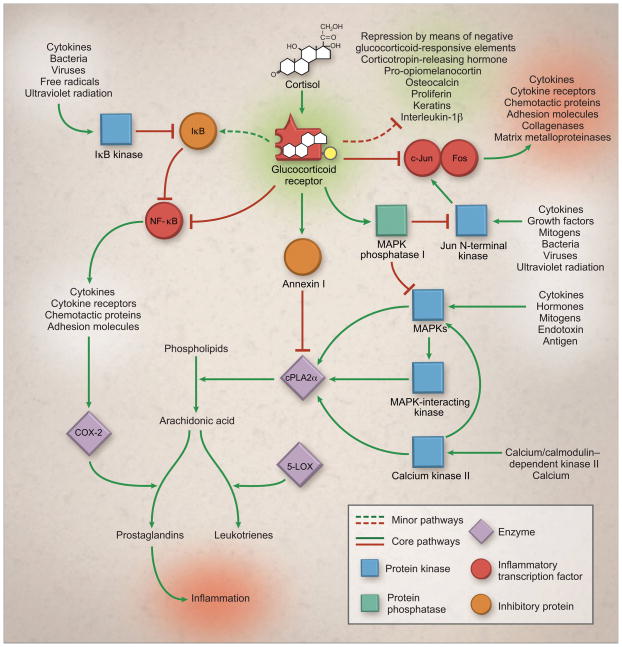
It has been recently demonstrated that interleukin 1β (IL-1β) plays a central role in monosodium urate crystal-induced inflammation and that the NALP3 inflammasome plays a major role in IL-1β production. These discoveries have offered new insights into the pathogenesis of acute gouty arthritis. In this review, we discuss the molecular mechanisms by which monosodium urate crystals induce acute inflammation and examine the mechanisms of action (MOAs) of traditional anti-inflammatory drugs (e.g., nonsteroidal anti-inflammatory drugs, colchicine, and glucocorticoids) and biologic agents (e.g., the IL-1β antagonists anakinra, rilonacept, and canakinumab) to understand how their MOAs contribute to their safety profiles. Traditional anti-inflammatory agents may act on the IL-1β pathway at some level; however, their MOAs are broad-ranging, unspecific, and biologically complex. This lack of specificity may explain the range of systemic adverse effects associated with them. The therapeutic margins of nonsteroidal anti-inflammatory drugs, colchicine, and glucocorticoids are particularly low in elderly patients and in patients with cardiovascular, metabolic, or renal comorbidities that are frequently associated with gouty arthritis. In contrast, the IL-1β antagonists act on very specific targets of inflammation, which may decrease the potential for systemic adverse effects, although infrequent but serious adverse events (including infection and administration reactions) have been reported. Because these IL-1β antagonists target an early event immediately downstream from NALP3 inflammasome activation, they may provide effective alternatives to traditional agents with minimal systemic adverse effects. Results of ongoing trials of IL-1β antagonists will likely provide clarification of their potential role in the management of acute gouty arthritis.
最近已经证明白细胞介素 1β(IL-1β)在单钠尿酸盐晶体诱导的炎症中起核心作用,并且 NALP3 炎性小体在 IL-1β产生中起主要作用。这些发现为急性痛风性关节炎的发病机制提供了新的见解。在这篇综述中,我们讨论了单钠尿酸盐晶体诱导急性炎症的分子机制,并研究了传统抗炎药物(例如非甾体抗炎药、秋水仙碱和糖皮质激素)和生物制剂(例如 IL-1β拮抗剂阿那白滞素、rilonacept 和 canakinumab)的作用机制,以了解其作用机制如何有助于它们的安全概况。传统的抗炎药可能在某种程度上作用于 IL-1β途径;然而,它们的作用机制广泛、非特异性且生物学上复杂。这种非特异性可能解释了与它们相关的全身性不良反应的范围。非甾体抗炎药、秋水仙碱和糖皮质激素在老年患者以及经常与痛风性关节炎相关的心血管、代谢或肾脏合并症患者中的治疗窗特别低。相比之下,IL-1β拮抗剂作用于炎症的非常特异的靶点,这可能降低全身性不良反应的可能性,尽管已经报道了罕见但严重的不良反应(包括感染和给药反应)。由于这些 IL-1β拮抗剂针对 NALP3 炎性小体激活后下游的早期事件,因此它们可能提供与传统药物相比具有最小全身性不良反应的有效替代方案。IL-1β拮抗剂的正在进行的试验结果可能会澄清它们在急性痛风性关节炎治疗中的潜在作用。