Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA.
J Cardiovasc Magn Reson. 2013 Jan 16;15(1):6. doi: 10.1186/1532-429X-15-6.
Echocardiography (echo) is a first line test to assess cardiac structure and function. It is not known if cardiovascular magnetic resonance (CMR) with late gadolinium enhancement (LGE) ordered during routine clinical practice in selected patients can add additional prognostic information after routine echo. We assessed whether CMR improves outcomes prediction after contemporaneous echo, which may have implications for efforts to optimize processes of care, assess effectiveness, and allocate limited health care resources.
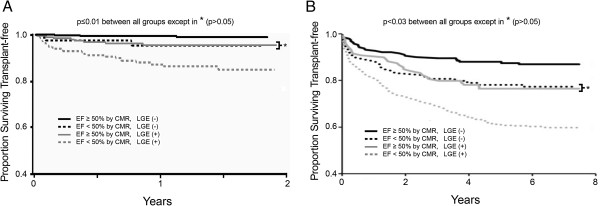
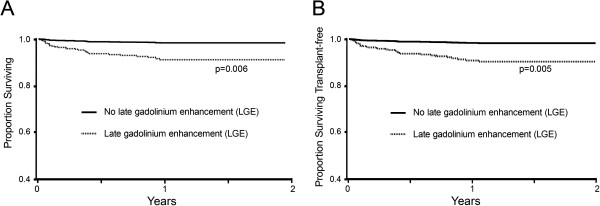
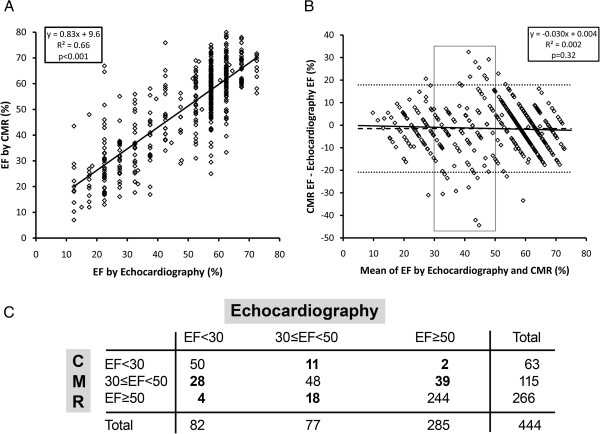
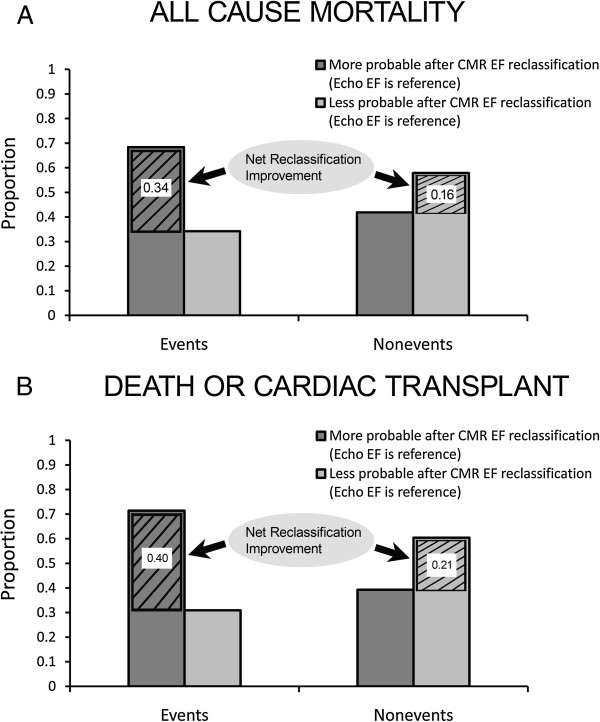
We prospectively enrolled 1044 consecutive patients referred for CMR. There were 38 deaths and 3 cardiac transplants over a median follow-up of 1.0 years (IQR 0.4-1.5). We first reproduced previous survival curve strata (presence of LGE and ejection fraction (EF) < 50%) for transplant free survival, to support generalizability of any findings. Then, in a subset (n = 444) with contemporaneous echo (median 3 days apart, IQR 1-9), EF by echo (assessed visually) or CMR were modestly correlated (R(2) = 0.66, p < 0.001), and 30 deaths and 3 transplants occurred over a median follow-up of 0.83 years (IQR 0.29-1.40). CMR EF predicted mortality better than echo EF in univariable Cox models (Integrated Discrimination Improvement (IDI) 0.018, 95% CI 0.008-0.034; Net Reclassification Improvement (NRI) 0.51, 95% CI 0.11-0.85). Finally, LGE further improved prediction beyond EF as determined by hazard ratios, NRI, and IDI in all Cox models predicting mortality or transplant free survival, adjusting for age, gender, wall motion, and EF.
Among those referred for CMR after echocardiography, CMR with LGE further improves risk stratification of individuals at risk for death or death/cardiac transplant.
超声心动图(echo)是评估心脏结构和功能的一线检查方法。尚不清楚在选定患者的常规临床实践中,是否可以在常规 echo 检查后,通过心血管磁共振(CMR)并结合晚期钆增强(LGE)检查来提供额外的预后信息。我们评估了在同期进行的 echo 检查后,CMR 是否可以改善预后预测,这可能对优化医疗流程、评估效果和分配有限的医疗资源产生影响。
我们前瞻性地纳入了 1044 例连续转诊至 CMR 的患者。在中位随访 1.0 年(IQR 0.4-1.5)期间,有 38 例死亡和 3 例心脏移植。我们首先复制了之前的生存曲线分层(有无 LGE 和射血分数(EF)<50%),以支持任何发现的可推广性。然后,在具有同期 echo(中位时间相差 3 天,IQR 1-9)的亚组(n=444)中,echo 评估的 EF(通过目测)或 CMR 有适度的相关性(R(2) = 0.66,p<0.001),中位随访 0.83 年(IQR 0.29-1.40)期间发生了 30 例死亡和 3 例移植。在单变量 Cox 模型中,CMR EF 比 echo EF 更能预测死亡率(综合判别改善(IDI)0.018,95%CI 0.008-0.034;净重新分类改善(NRI)0.51,95%CI 0.11-0.85)。最后,在所有预测死亡率或无移植生存的 Cox 模型中,LGE 均通过危险比、NRI 和 IDI 进一步改善 EF 的预测,这些模型还调整了年龄、性别、壁运动和 EF。
在 echocardiography 后接受 CMR 检查的患者中,CMR 并结合 LGE 进一步改善了死亡或死亡/心脏移植风险患者的风险分层。