Department of Urology, Wonkwang University School of Medicine & Hospital, Iksan, Korea.
Int Neurourol J. 2012 Dec;16(4):175-80. doi: 10.5213/inj.2012.16.4.175. Epub 2012 Dec 31.
Triple therapy with gabapentin, amitriptyline, and nonsteroidal antiinflammatory drugs is efficacious for chronic bladder pain syndrome/interstitial cystitis (BPS/IC). However, transient, fluctuating, worsening pain or flare-up symptoms may develop during treatment for a variety of reasons. Here, we assessed the validity of our observational experience regarding a short course of oral prednisolone therapy, which might be of value in the management of flare-up symptoms of BPS/IC.
Between May 2007 and May 2012, 7 women (mean age, 61.5 years; range, 44.8 to 75.4 years) with BPS/IC presenting with transient, fluctuating, worsening pain as a flare-up symptom despite low-dose triple therapy received a 1- to 3-month course of oral prednisolone 10 mg. The outcome measures used were the IC symptom scale (ICSS, O'Leary-Sant Interstitial Cystitis Symptom Index) and a visual analogue scale (VAS), which were completed at baseline and after treatment.
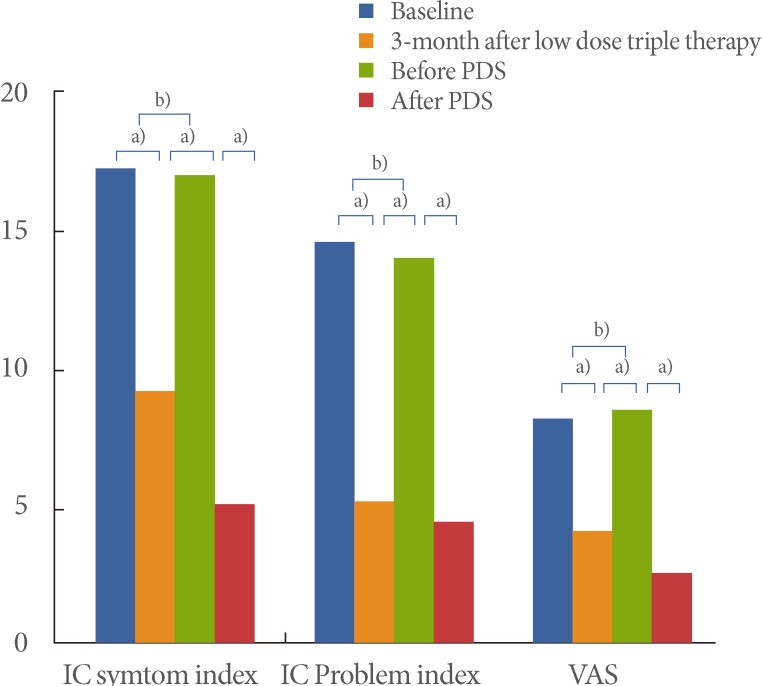
There were statistically significant differences in the ICSS and VAS score before and after prednisolone treatment (P<0.05 by Wilcoxon singed-rank test). The pretreatment IC symptom index (ICSI), IC problem index (ICPI), and VAS score were 16.7± 2.2, 13.7±2.3, and 8.3±1.5 (mean±standard deviation [SD]), and the posttreatment scores were 4.9±2.3, 4.3±1.1, and 2.5±0.9 (mean±SD), respectively. The ICSI, ICPI, and VAS scores were improved after prednisolone treatment by 70.7%, 68.6%, and 69.9%, respectively. Low-dose triple therapy with prednisolone caused no significant adverse effects.
In patients with BPS/IC who show transient, fluctuating, worsening pain as flare-up symptoms despite undergoing low-dose triple therapy, a short course of oral prednisolone therapy was sufficiently effective. However, large-scale studies should be performed to verify our findings.
加巴喷丁、阿米替林和非甾体抗炎药三联疗法对慢性膀胱疼痛综合征/间质性膀胱炎(BPS/IC)有效。然而,由于各种原因,在治疗过程中可能会出现短暂、波动、加重的疼痛或发作症状。在这里,我们评估了我们关于短期口服泼尼松治疗的观察经验的有效性,这可能对 BPS/IC 发作症状的管理有价值。
在 2007 年 5 月至 2012 年 5 月期间,7 名(平均年龄 61.5 岁;范围 44.8 至 75.4 岁)患有 BPS/IC 的女性患者出现短暂、波动、加重的疼痛作为发作症状,尽管接受了低剂量三联疗法,但仍接受了 1 至 3 个月的口服泼尼松 10mg 治疗。使用的结局测量指标为 IC 症状量表(ICSS,O'Leary-Sant 间质性膀胱炎症状指数)和视觉模拟量表(VAS),在基线和治疗后完成。
泼尼松治疗前后 ICSS 和 VAS 评分有统计学差异(Wilcoxon 符号秩检验 P<0.05)。治疗前 IC 症状指数(ICSI)、IC 问题指数(ICPI)和 VAS 评分分别为 16.7±2.2、13.7±2.3 和 8.3±1.5(平均值±标准差[SD]),治疗后评分分别为 4.9±2.3、4.3±1.1 和 2.5±0.9(平均值±SD)。泼尼松治疗后 ICSI、ICPI 和 VAS 评分分别改善了 70.7%、68.6%和 69.9%。低剂量三联疗法加用泼尼松治疗无明显不良反应。
对于接受低剂量三联疗法后仍出现短暂、波动、加重的疼痛作为发作症状的 BPS/IC 患者,短期口服泼尼松治疗是有效的。然而,应进行大规模研究来验证我们的发现。