Mère et enfant face aux infections tropicales, IRD unité mixte de recherche 216, Université Paris Descartes-Paris V, 4 avenue de l'Observatoire, Paris Cedex 06 75270, France.
Malar J. 2013 Jan 25;12:35. doi: 10.1186/1475-2875-12-35.
Chloroquine (CQ) was the main malaria therapy worldwide from the 1940s until the 1990s. Following the emergence of CQ-resistant Plasmodium falciparum, most African countries discontinued the use of CQ, and now promote artemisinin-based combination therapy as the first-line treatment. This change was generally initiated during the last decade in West and Central Africa. The aim of this study is to describe the changes in CQ susceptibility in this African region, using travellers returning from this region as a sentinel system.
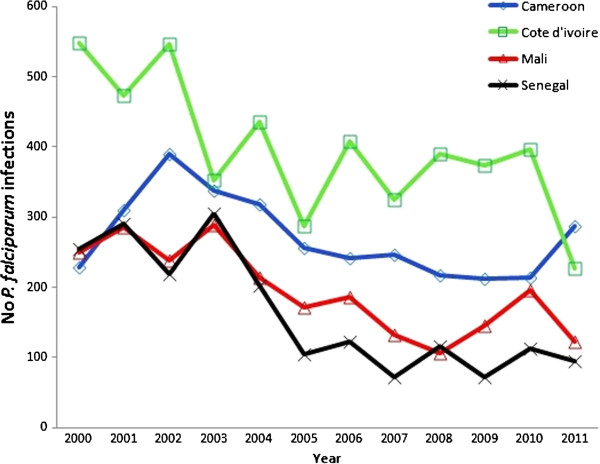
The study was conducted by the Malaria National Reference Centre, France. The database collated the pfcrtK76T molecular marker for CQ susceptibility and the in vitro response to CQ of parasites from travellers' isolates returning from Senegal, Mali, Ivory Coast or Cameroon. As a proxy of drug pressure, data regarding CQ intake in febrile children were collated for the study period. Logistic regression models were used to detect trends in the proportions of CQ resistant isolates.
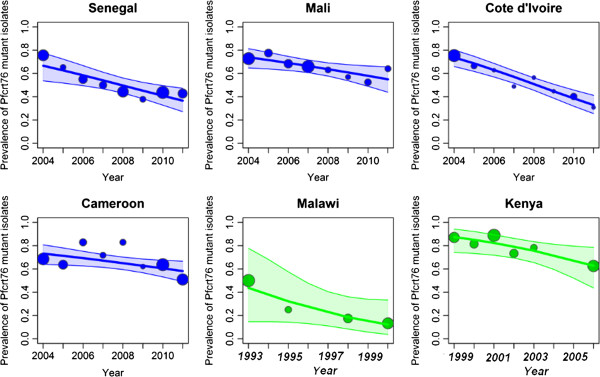
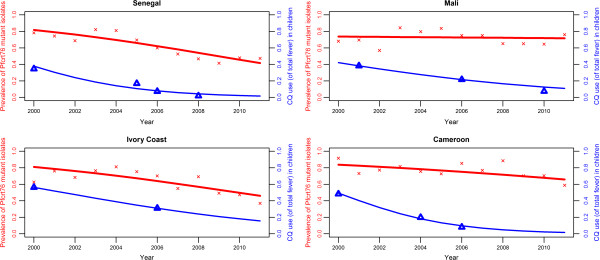
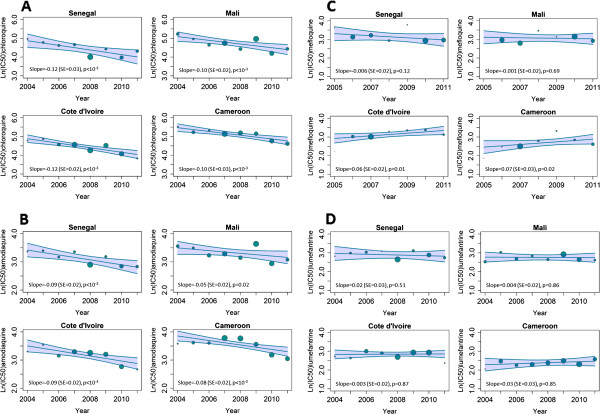
A total of 2874 parasite isolates were genotyped between 2000-2011. The prevalence of the pfcrt76T mutant genotype significantly decreased for Senegal (from 78% to 47%), Ivory Coast (from 63% to 37%), Cameroon (from 90% to 59%) and remained stable for Mali. The geometric mean of the 50% inhibitory concentration (IC50) of CQ in vitro susceptibility and the proportion of resistant isolates (defining resistance as an IC50 value > 100 nM) significantly decreased for Senegal (from 86 nM (59%) to 39 nM (25%)), Mali (from 84 nM (50%) to 51 nM (31%)), Ivory Coast (from 75 nM (59%) to 29 nM (16%)) and Cameroon (from 181 nM (75%) to 51 nM (37%)). Both analyses (molecular and in vitro susceptibility) were performed for the 2004-2011 period, after the four countries had officially discontinued CQ and showed an accelerated decline of the resistant isolates for the four countries. Meanwhile, CQ use among children significantly deceased in this region (fixed effects slope = -0.3, p < 10-3).
An increase in CQ susceptibility following official withdrawal of the drug was observed in travellers returning from West and Central African countries. The same trends were observed for molecular and in vitro analysis between 2004-2011 and they correlated to the decrease of the drug pressure.
从 20 世纪 40 年代到 90 年代,氯喹(CQ)是世界范围内治疗疟疾的主要药物。随着耐 CQ 的恶性疟原虫的出现,大多数非洲国家停止使用 CQ,现在提倡青蒿素为基础的联合疗法作为一线治疗。这一变化通常在上个十年在西非和中非开始。本研究的目的是描述该地区 CQ 敏感性的变化,使用从该地区返回的旅行者作为监测系统。
该研究由法国疟疾国家参考中心进行。该数据库收集了旅行者从塞内加尔、马里、科特迪瓦或喀麦隆返回时寄生虫的 pfcrtK76T 分子标记,以确定 CQ 敏感性,以及体外对 CQ 的反应。作为药物压力的替代指标,收集了研究期间发热儿童 CQ 摄入的数据。使用逻辑回归模型检测 CQ 耐药分离株比例的趋势。
2000 年至 2011 年间共对 2874 株寄生虫分离株进行了基因分型。塞内加尔(从 78%降至 47%)、科特迪瓦(从 63%降至 37%)和喀麦隆(从 90%降至 59%)pfcrt76T 突变基因型的流行率显著下降,马里保持稳定。体外 CQ 敏感性的半数抑制浓度(IC50)的几何平均值和耐药分离株的比例(将 IC50 值>100 nM 定义为耐药)在塞内加尔(从 86 nM(59%)降至 39 nM(25%))、马里(从 84 nM(50%)降至 51 nM(31%))、科特迪瓦(从 75 nM(59%)降至 29 nM(16%))和喀麦隆(从 181 nM(75%)降至 51 nM(37%))显著降低。在这四个国家正式停止使用 CQ 后,对 2004 年至 2011 年期间进行了分子和体外敏感性分析,显示这四个国家的耐药分离株数量迅速减少。同时,该地区儿童使用 CQ 的情况显著减少(固定效应斜率=-0.3,p<0.001)。
在从西非和中非国家返回的旅行者中,观察到官方停止使用该药物后 CQ 敏感性增加。2004 年至 2011 年期间,分子和体外分析也观察到了相同的趋势,与药物压力的下降相关。