Hofhuis José G M, van Stel Henk F, Schrijvers Augustinus J P, Rommes Johannes H, Spronk Peter E
Crit Care. 2013 Jan 28;17(1):R17. doi: 10.1186/cc12491.
Acute kidney injury (AKI) is a serious complication in critically ill patients admitted to the Intensive Care Unit (ICU). We hypothesized that ICU survivors with AKI would have a worse health-related quality of life (HRQOL) outcome than ICU survivors without AKI.
We performed a long-term prospective observational study. Patients admitted for > 48 hours in a medical-surgical ICU were included and divided in two groups: patients who fulfilled RIFLE criteria for AKI and patients without AKI. We used the Short-Form 36 to evaluate HRQOL before admission (by proxy within 48 hours after admission of the patient), at ICU discharge, hospital discharge, 3 and 6 months following ICU discharge (all by patients). Recovery in HRQOL from ICU-admission onwards was assessed using linear mixed modelling.
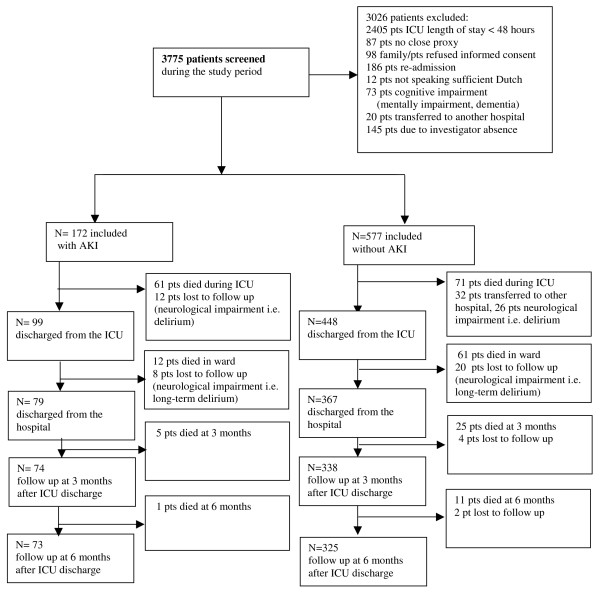
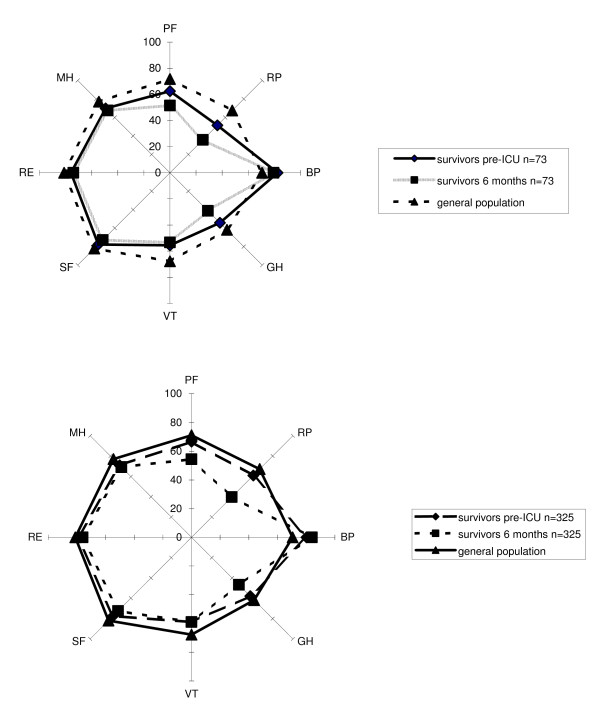
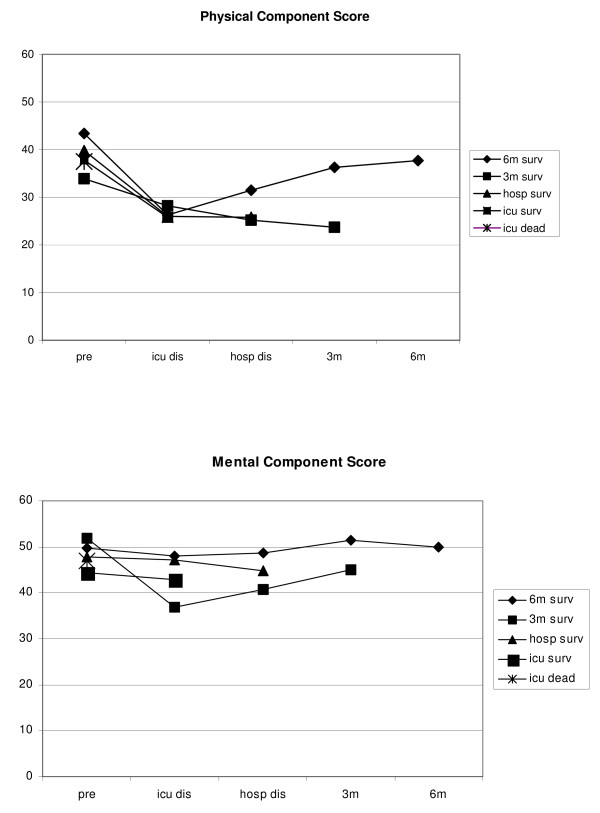
Between September 2000 and January 2007 all admissions were screened for study participation. We included a total of 749 patients. At six months after ICU discharge 73 patients with AKI and 325 patients without AKI could be evaluated. In survivors with and without AKI, the pre-admission HRQOL (by proxy) and at six months after ICU discharge was significantly lower compared with an age matched general population. Most SF-36 dimensions changed significantly over time from ICU discharge. Change over time of HRQOL between the different AKI Rifle classes (Risk, Injury, Failure) showed no significant differences. At ICU discharge, scores were lowest in the group with AKI compared with the group without AKI for the physical functioning, role-physical and general health dimensions. However, there were almost no differences in HRQOL between both groups at six months.
The pre-admission HRQOL (by proxy) of AKI survivors was significantly lower in two dimensions compared with the age matched general population. Six months after ICU discharge survivors with and without AKI showed an almost similar HRQOL. However, compared with the general population with a similar age, HRQOL was poorer in both groups.
急性肾损伤(AKI)是入住重症监护病房(ICU)的危重症患者的一种严重并发症。我们假设,与未发生AKI的ICU幸存者相比,发生AKI的ICU幸存者的健康相关生活质量(HRQOL)结局更差。
我们进行了一项长期前瞻性观察研究。纳入在内科-外科ICU住院超过48小时的患者,并将其分为两组:符合AKI的RIFLE标准的患者和未发生AKI的患者。我们使用简短健康调查问卷(Short-Form 36)在入院前(在患者入院后48小时内由代理人填写)、ICU出院时、医院出院时、ICU出院后3个月和6个月(均由患者本人填写)评估HRQOL。使用线性混合模型评估从入院到ICU出院后HRQOL的恢复情况。
在2000年9月至2007年1月期间,对所有入院患者进行了研究参与筛查。我们共纳入了749例患者。在ICU出院后6个月时,可对73例发生AKI的患者和325例未发生AKI的患者进行评估。在发生和未发生AKI的幸存者中,入院前(由代理人填写)和ICU出院后6个月时的HRQOL与年龄匹配的普通人群相比显著更低。从ICU出院起,大多数SF-36维度随时间发生了显著变化。不同AKI Rifle分级(风险、损伤、衰竭)之间HRQOL随时间的变化无显著差异。在ICU出院时,在身体功能、角色-身体和总体健康维度方面,发生AKI的组与未发生AKI的组相比得分最低。然而,两组在6个月时的HRQOL几乎没有差异。
与年龄匹配的普通人群相比,AKI幸存者入院前(由代理人填写)的HRQOL在两个维度上显著更低。在ICU出院后6个月,发生和未发生AKI的幸存者的HRQOL几乎相似。然而,与年龄相似的普通人群相比,两组的HRQOL均较差。