Department of General, Gastroenterological and Oncological Surgery, Medical University of Warsaw, ul. Banacha 1A, 02-097 Warsaw, Poland.
Surg Endosc. 2013 Aug;27(8):2841-8. doi: 10.1007/s00464-013-2831-9. Epub 2013 Feb 13.
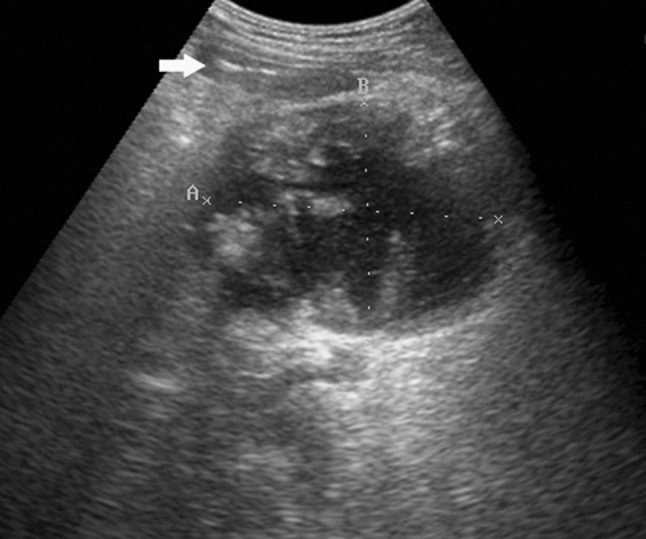
The role of percutaneous drainage in the management of infected pancreatic necrosis remains controversial, and ultrasound-guided technique is rarely used for this indication. The purpose of this study was to evaluate the safety and efficacy of sonographically guided percutaneous catheter drainage for infected pancreatic necrosis.
The patient group consisted of 16 men and 2 women. The mean age of the patients was 47 years. The median computed tomography severity index of acute pancreatitis was 10 points. Percutaneous catheter drainage was performed under sonographic guidance using preferably retroperitoneal approach, and transperitoneal access in selected cases. The medical records and imaging scans were reviewed retrospectively for each patient.
Percutaneous catheter drainage resulted in a complete resolution of infected pancreatic necrosis in 6 of 18 patients (33 %). Twelve of 18 patients who were initially managed with PCD required eventually necrosectomy (67 %). The most common reason for crossover to surgical intervention was persistent sepsis (n = 7). Open necrosectomy was performed in 4 of these patients, and 3 patients underwent successful minimally invasive retroperitoneal necrosectomy. Five patients required conversion to open surgery because of procedure-related complications. In 3 cases, there was leakage of the necrotic material into the peritoneal cavity. Two other patients experienced hemorrhagic complications. Overall mortality rate was 17 %. The size of the largest necrotic collection in patients who were successfully treated with percutaneous drainage decreased by a median of 76 % shortly after the procedure, whereas it decreased only by a median of 16 % in cases of failure of percutaneous drainage.
Ultrasound-guided percutaneous catheter drainage used in infected pancreatic necrosis is a technique with acceptably low morbidity and mortality that may be the definitive treatment or a bridge management to necrosectomy. A negligible decrease in size of the necrotic collection predicts failure of percutaneous drainage.
经皮引流在感染性胰腺坏死治疗中的作用仍存在争议,且超声引导技术很少用于该适应证。本研究旨在评估超声引导下经皮导管引流治疗感染性胰腺坏死的安全性和有效性。
患者组包括 16 名男性和 2 名女性。患者的平均年龄为 47 岁。急性胰腺炎的中位 CT 严重指数为 10 分。经皮导管引流在超声引导下进行,首选腹膜后入路,在选择的病例中采用腹膜下入路。回顾性分析每位患者的病历和影像学扫描。
18 例患者中,6 例(33%)经皮导管引流使感染性胰腺坏死完全消退。12 例最初接受 PCD 治疗的患者最终需要行坏死组织清除术(67%)。交叉到手术干预的最常见原因是持续性败血症(n=7)。其中 4 例行开放性坏死组织清除术,3 例行成功的微创腹膜后坏死组织清除术。5 例患者因与操作相关的并发症而转为开放性手术。在 3 例中,坏死物质漏入腹腔。另外 2 例患者发生出血并发症。总的死亡率为 17%。在成功接受经皮引流治疗的患者中,最大坏死性积聚的大小在治疗后短期内中位数下降了 76%,而在经皮引流治疗失败的病例中仅中位数下降了 16%。
超声引导下经皮导管引流用于感染性胰腺坏死是一种具有可接受的低发病率和死亡率的技术,可能是确定性治疗或坏死组织清除术的桥接治疗。坏死性积聚大小的微小减少预示着经皮引流治疗的失败。