Laboratory of Renal Pathophysiology, LIM-16, Renal Division, Department of Clinical Medicine, Faculty of Medicine, University of São Paulo, São Paulo, Brazil.
PLoS One. 2013;8(2):e56215. doi: 10.1371/journal.pone.0056215. Epub 2013 Feb 19.
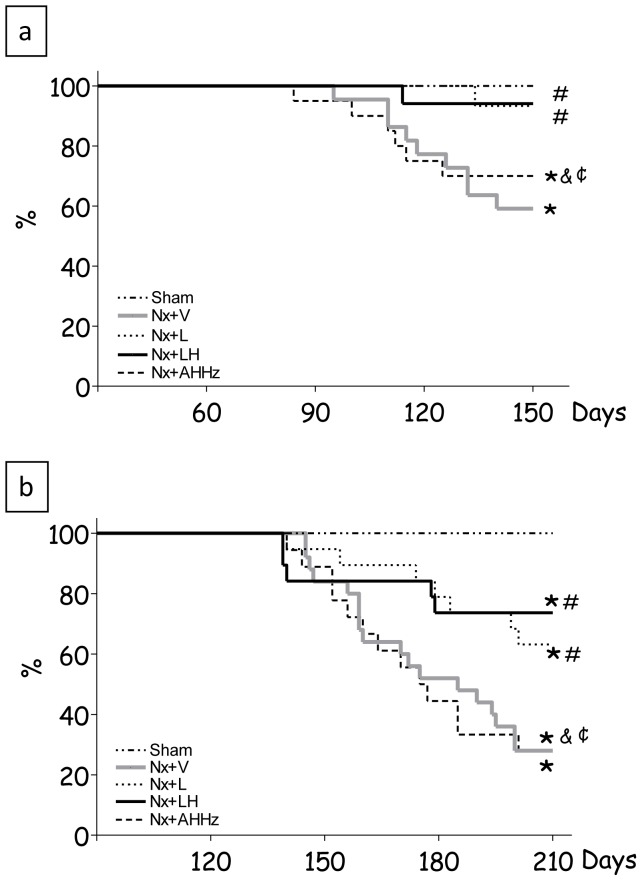
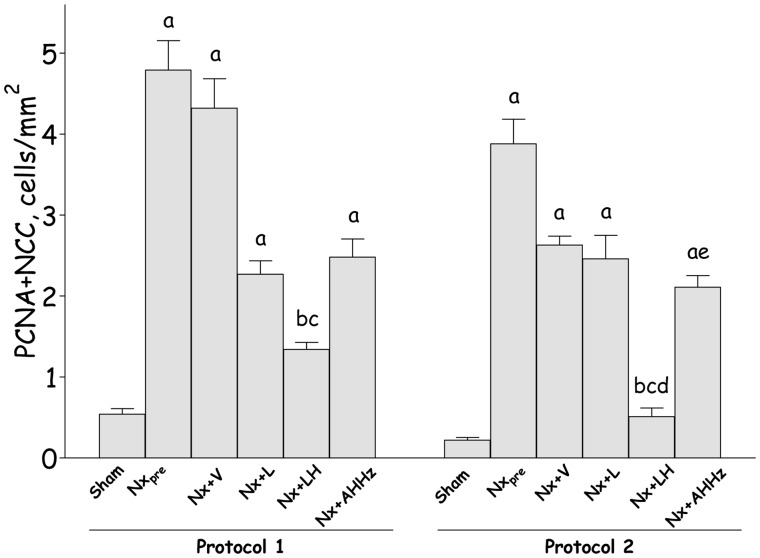
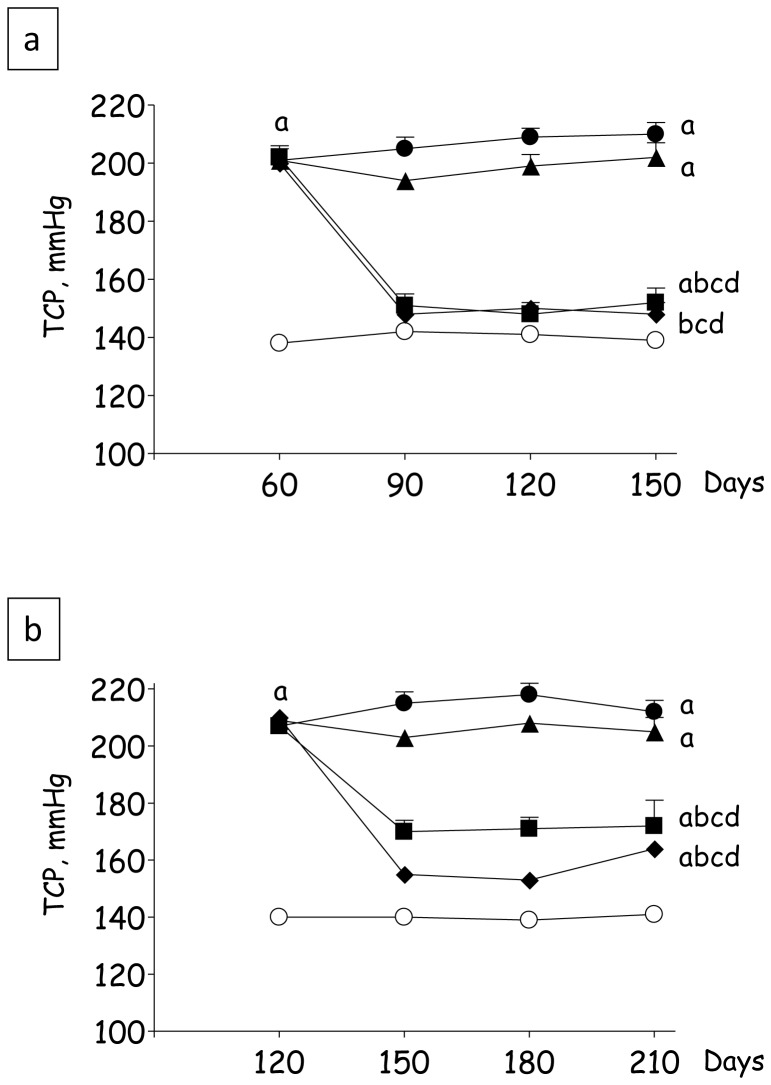
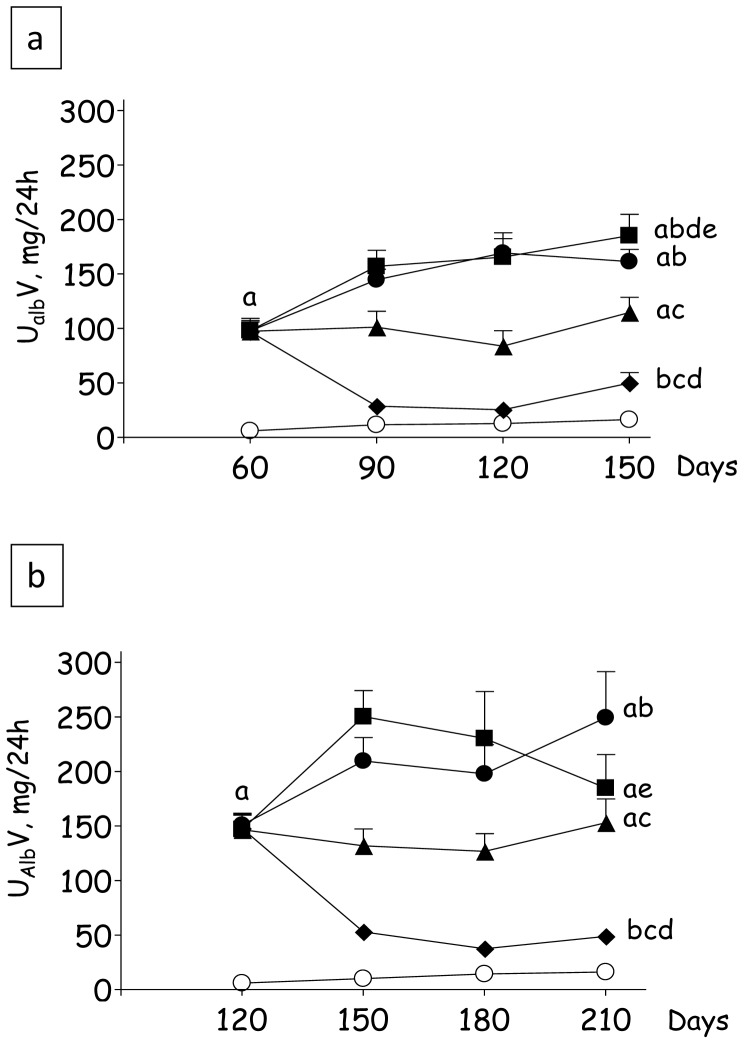
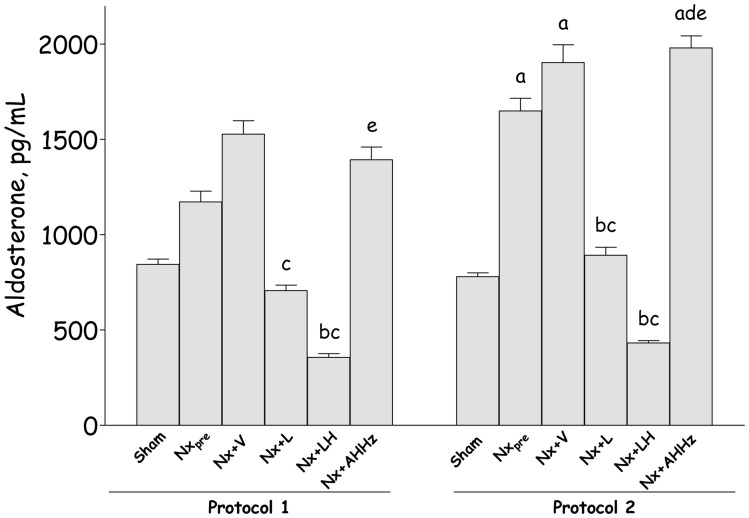
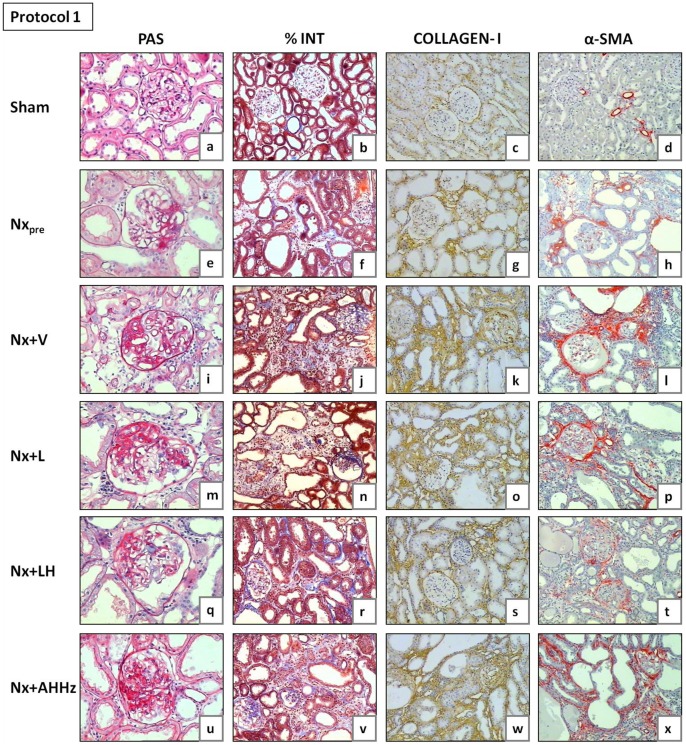
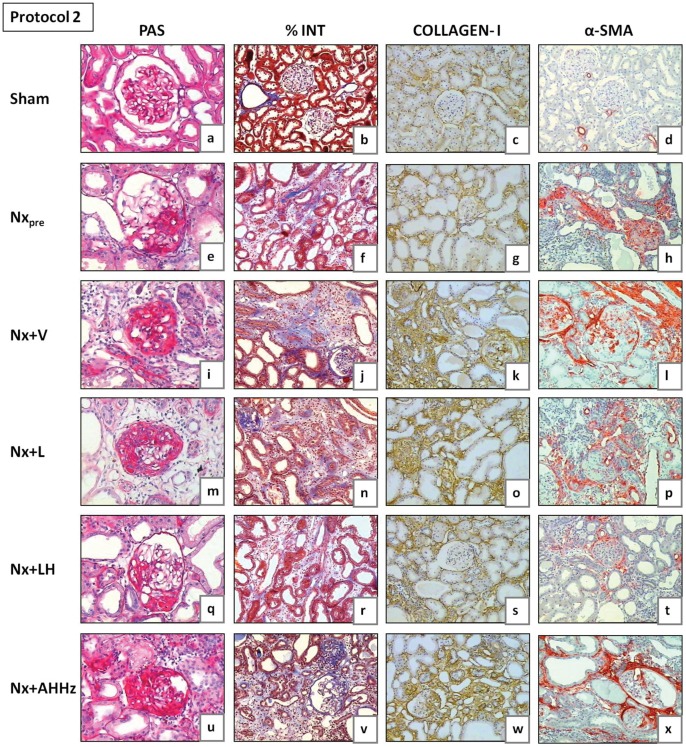
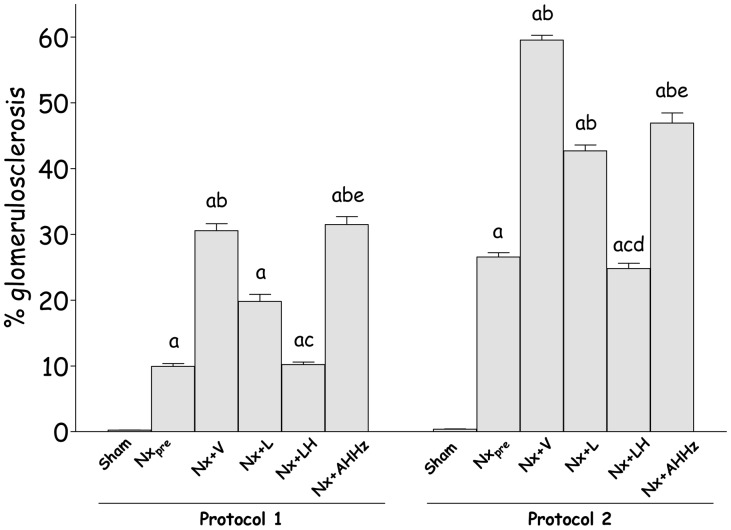
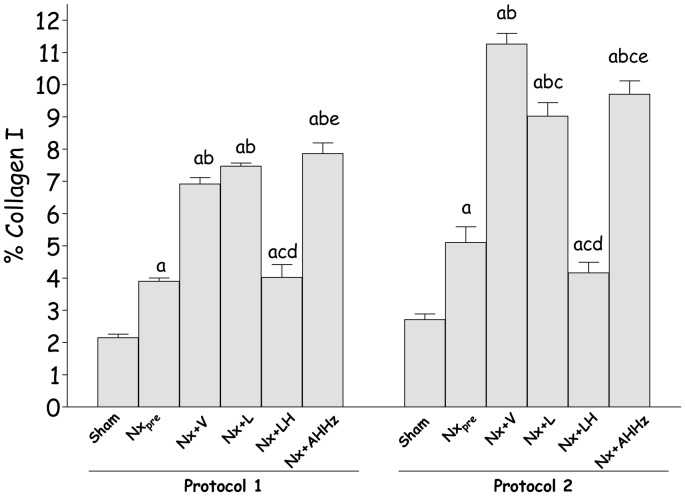
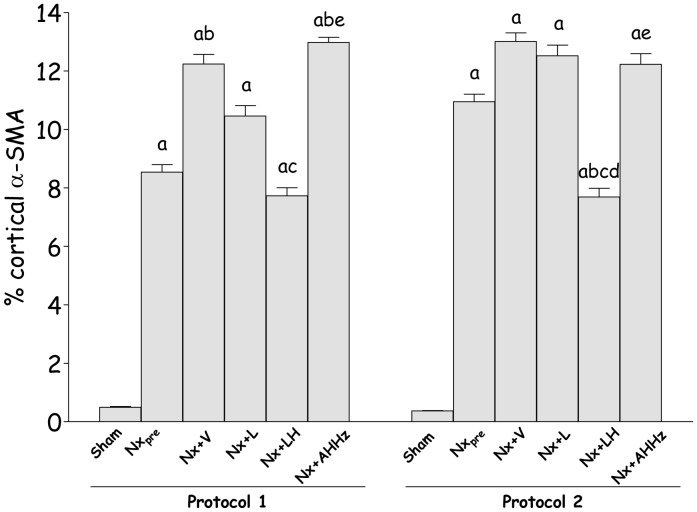
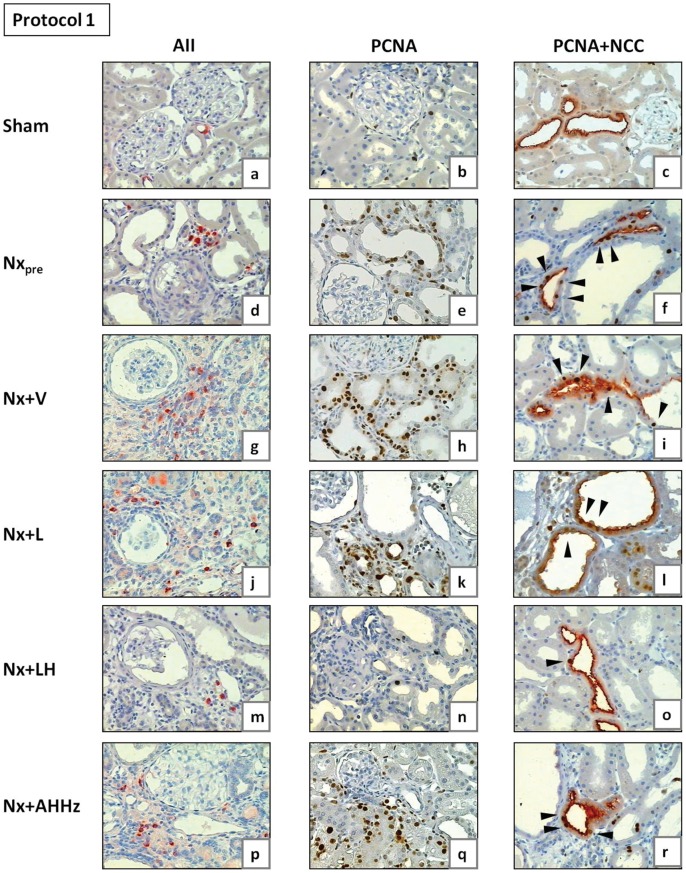
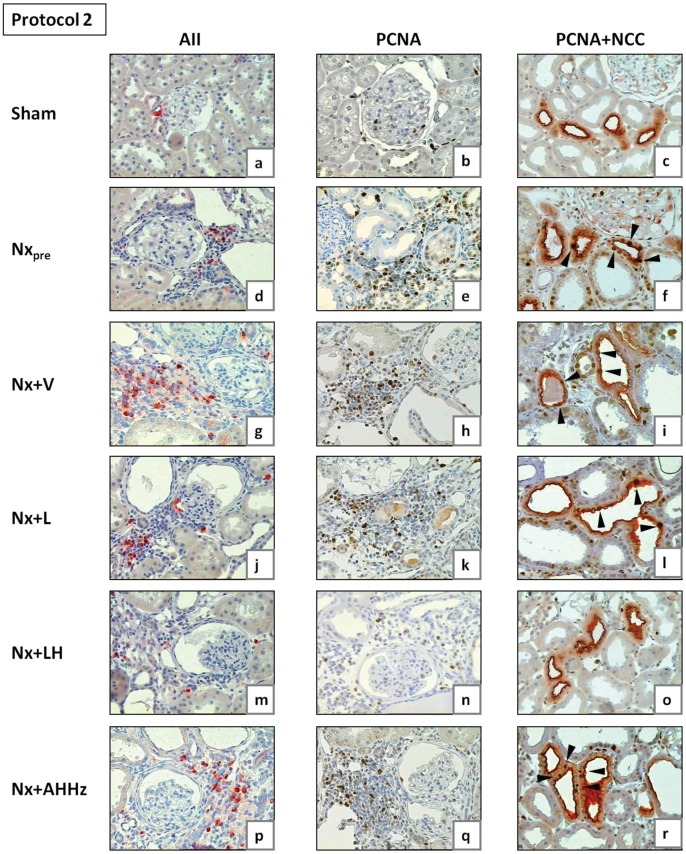
Treatments that effectively prevent chronic kidney disease (CKD) when initiated early often yield disappointing results when started at more advanced phases. We examined the long-term evolution of renal injury in the 5/6 nephrectomy model (Nx) and the effect of an association between an AT-1 receptor blocker, losartan (L), and hydrochlorothiazide (H), shown previously to be effective when started one month after Nx. Adult male Munich-Wistar rats underwent Nx, being divided into four groups: Nx+V, no treatment; Nx+L, receiving L monotherapy; Nx+LH, receiving the L+H association (LH), and Nx+AHHz, treated with the calcium channel blocker, amlodipine, the vascular relaxant, hydralazine, and H. This latter group served to assess the effect of lowering blood pressure (BP). Rats undergoing sham nephrectomy (S) were also studied. In a first protocol, treatments were initiated 60 days after Nx, when CKD is at a relatively early stage. In a second protocol, treatments were started 120 days after Nx, when glomerulosclerosis and interstitial fibrosis are already advanced. In both protocols, L treatment promoted only partial renoprotection, whereas LH brought BP, albuminuria, tubulointerstitial cell proliferation and plasma aldosterone below pretreatment levels, and completely detained progression of renal injury. Despite normalizing BP, the AHHz association failed to prevent renal damage, indicating that the renoprotective effect of LH was not due to a systemic hemodynamic action. These findings are inconsistent with the contention that thiazides are innocuous in advanced CKD. In Nx, LH promotes effective renoprotection even at advanced stages by mechanisms that may involve anti-inflammatory and intrarenal hemodynamic effects, but seem not to require BP normalization.
当在早期开始时,能有效预防慢性肾病(CKD)的治疗方法,在更晚期开始时往往效果不佳。我们研究了 5/6 肾切除术模型(Nx)中肾脏损伤的长期演变,以及血管紧张素受体阻滞剂氯沙坦(L)和氢氯噻嗪(H)联合治疗的效果,之前的研究表明,在 Nx 后一个月开始联合治疗是有效的。成年雄性慕尼黑-维斯塔大鼠接受 Nx,分为四组:Nx+V,不治疗;Nx+L,接受 L 单药治疗;Nx+LH,接受 L+H 联合治疗(LH),Nx+AHHz,用钙通道阻滞剂氨氯地平、血管扩张剂肼屈嗪和 H 治疗。后者组用于评估降低血压(BP)的效果。还研究了接受假手术(S)的大鼠。在第一个方案中,治疗在 Nx 后 60 天开始,此时 CKD 处于相对早期阶段。在第二个方案中,治疗在 Nx 后 120 天开始,此时肾小球硬化和间质纤维化已经很严重。在两个方案中,L 治疗仅促进部分肾脏保护,而 LH 使 BP、白蛋白尿、肾小管间质细胞增殖和血浆醛固酮恢复到治疗前水平,并完全阻止肾脏损伤的进展。尽管 AHHz 联合治疗能使血压正常化,但未能预防肾脏损伤,表明 LH 的肾脏保护作用不是由于全身血液动力学作用。这些发现与噻嗪类药物在晚期 CKD 中无害的观点不一致。在 Nx 中,LH 通过可能涉及抗炎和肾内血液动力学作用的机制,即使在晚期也能有效促进肾脏保护,而似乎不需要血压正常化。