School of Health Sciences, City University London, London EC1A 7QN, UK.
BMJ. 2013 Feb 26;346:f653. doi: 10.1136/bmj.f653.
To assess the effect of second generation, home based telehealth on health related quality of life, anxiety, and depressive symptoms over 12 months in patients with long term conditions.
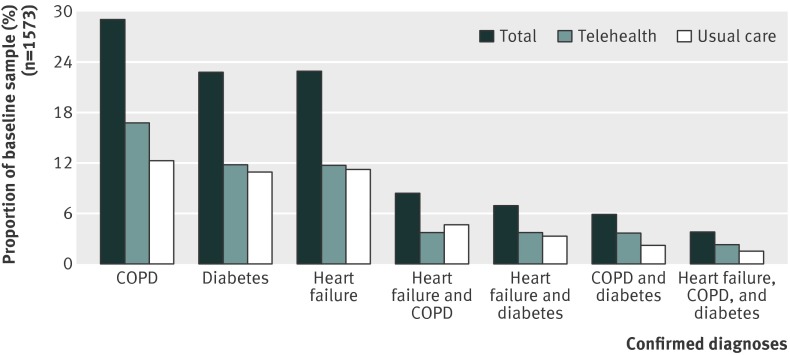
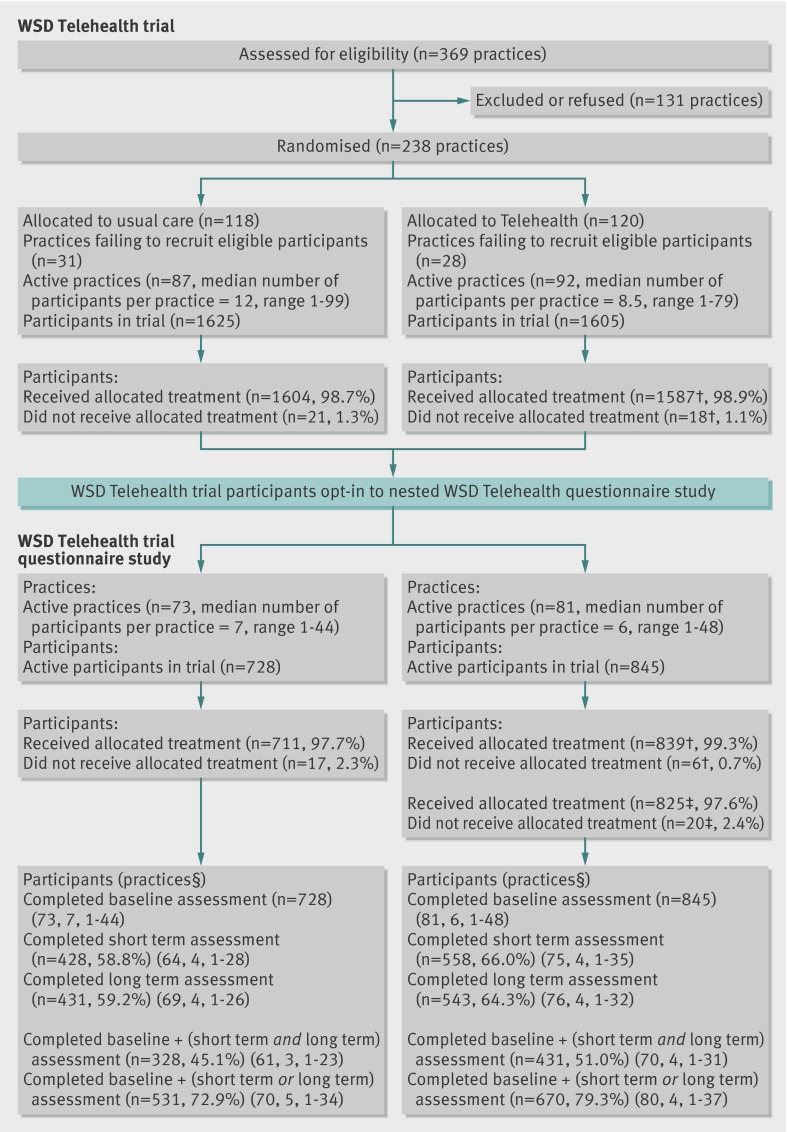
A study of patient reported outcomes (the Whole Systems Demonstrator telehealth questionnaire study; baseline n=1573) was nested in a pragmatic, cluster randomised trial of telehealth (the Whole Systems Demonstrator telehealth trial, n=3230). General practice was the unit of randomisation, and telehealth was compared with usual care. Data were collected at baseline, four months (short term), and 12 months (long term). Primary intention to treat analyses tested treatment effectiveness; multilevel models controlled for clustering by general practice and a range of covariates. Analyses were conducted for 759 participants who completed questionnaire measures at all three time points (complete case cohort) and 1201 who completed the baseline assessment plus at least one other assessment (available case cohort). Secondary per protocol analyses tested treatment efficacy and included 633 and 1108 participants in the complete case and available case cohorts, respectively.
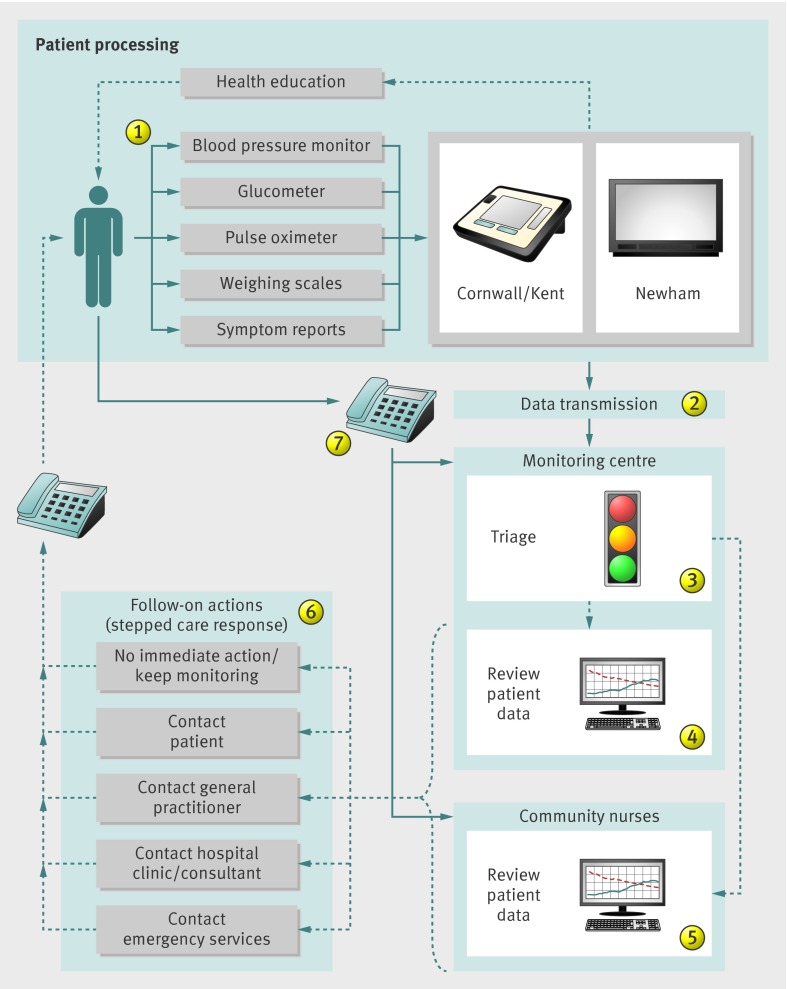
Provision of primary and secondary care via general practices, specialist nurses, and hospital clinics in three diverse regions of England (Cornwall, Kent, and Newham), with established integrated health and social care systems.
Patients with chronic obstructive pulmonary disease (COPD), diabetes, or heart failure recruited between May 2008 and December 2009.
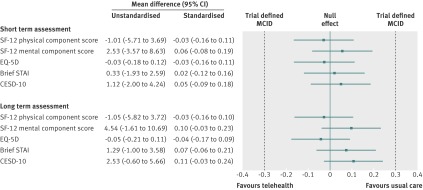
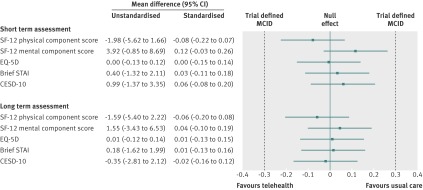
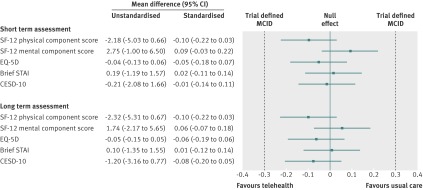
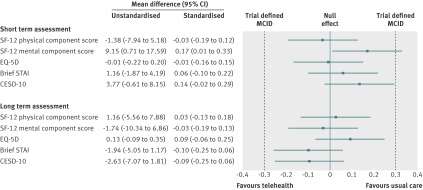
Generic, health related quality of life (assessed by physical and mental health component scores of the SF-12, and the EQ-5D), anxiety (assessed by the six item Brief State-Trait Anxiety Inventory), and depressive symptoms (assessed by the 10 item Centre for Epidemiological Studies Depression Scale).
In the intention to treat analyses, differences between treatment groups were small and non-significant for all outcomes in the complete case (0.480 ≤ P ≤ 0.904) or available case (0.181 ≤ P ≤ 0.905) cohorts. The magnitude of differences between trial arms did not reach the trial defined, minimal clinically important difference (0.3 standardised mean difference) for any outcome in either cohort at four or 12 months. Per protocol analyses replicated the primary analyses; the main effect of trial arm (telehealth v usual care) was non-significant for any outcome (complete case cohort 0.273 ≤ P ≤ 0.761; available case cohort 0.145 ≤ P ≤ 0.696).
Second generation, home based telehealth as implemented in the Whole Systems Demonstrator Evaluation was not effective or efficacious compared with usual care only. Telehealth did not improve quality of life or psychological outcomes for patients with chronic obstructive pulmonary disease, diabetes, or heart failure over 12 months. The findings suggest that concerns about potentially deleterious effect of telehealth are unfounded for most patients.
ISRCTN43002091.
评估第二代家庭远程医疗对患有长期疾病的患者在 12 个月内的健康相关生活质量、焦虑和抑郁症状的影响。
对患者报告的结果进行了一项研究(整个系统演示者远程医疗问卷研究;基线 n=1573),嵌套在远程医疗的实用、群组随机试验中(整个系统演示者远程医疗试验,n=3230)。普通实践是随机分组的单位,远程医疗与常规护理进行了比较。数据在基线、四个月(短期)和 12 个月(长期)时收集。主要意向治疗分析测试了治疗效果;多层次模型控制了普通实践的聚类和一系列协变量。对完成所有三个时间点问卷调查的 759 名参与者(完整案例队列)和完成基线评估且至少完成其他一项评估的 1201 名参与者(可用案例队列)进行了分析。次要的按方案分析测试了治疗效果,并分别包括完整案例和可用案例队列中的 633 名和 1108 名参与者。
通过普通实践、专科护士和英格兰三个不同地区(康沃尔、肯特和纽汉姆)的医院诊所提供初级和二级护理,这些地区都有成熟的综合卫生和社会保健系统。
2008 年 5 月至 2009 年 12 月期间招募的慢性阻塞性肺疾病(COPD)、糖尿病或心力衰竭患者。
一般健康相关的生活质量(通过 SF-12 的身体和心理健康组成部分评分以及 EQ-5D 评估)、焦虑(通过 6 项简短状态特质焦虑量表评估)和抑郁症状(通过 10 项流行病学研究中心抑郁量表评估)。
在意向治疗分析中,在完整案例(0.480≤P≤0.904)或可用案例(0.181≤P≤0.905)队列中,治疗组之间的差异较小且不显著。在任何一个队列中,在四个月或 12 个月时,试验臂之间的差异幅度都没有达到试验定义的最小临床重要差异(0.3 个标准化均数差异)。方案分析复制了主要分析;试验臂(远程医疗与常规护理)的主要效果在任何结局上均不显著(完整案例队列 0.273≤P≤0.761;可用案例队列 0.145≤P≤0.696)。
与常规护理相比,在整个系统演示器评估中实施的第二代家庭远程医疗并没有效果或疗效。在 12 个月内,远程医疗并没有改善 COPD、糖尿病或心力衰竭患者的生活质量或心理结局。这些发现表明,对于大多数患者来说,对远程医疗可能产生有害影响的担忧是没有根据的。
ISRCTN43002091。