Department of General Surgery, Wake Forest School of Medicine, Winston-Salem, NC, USA.
Ann Surg Oncol. 2013 Apr;20(4):1088-92. doi: 10.1245/s10434-012-2787-3. Epub 2013 Mar 2.
Cytoreductive surgery (CS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is the treatment most likely to achieve prolonged survival in peritoneal carcinomatosis (PC). Yet the efficacy of HIPEC in rectal patients is controversial because of the retroperitoneal location of the primary tumor. Therefore, we reviewed our experience in patients with PC from a rectal primary tumor.
A retrospective analysis of a prospective database of 950 HIPEC procedures was performed. Performance status, age, albumin level, prior surgical score, resection status, morbidity, mortality, and survival were reviewed.
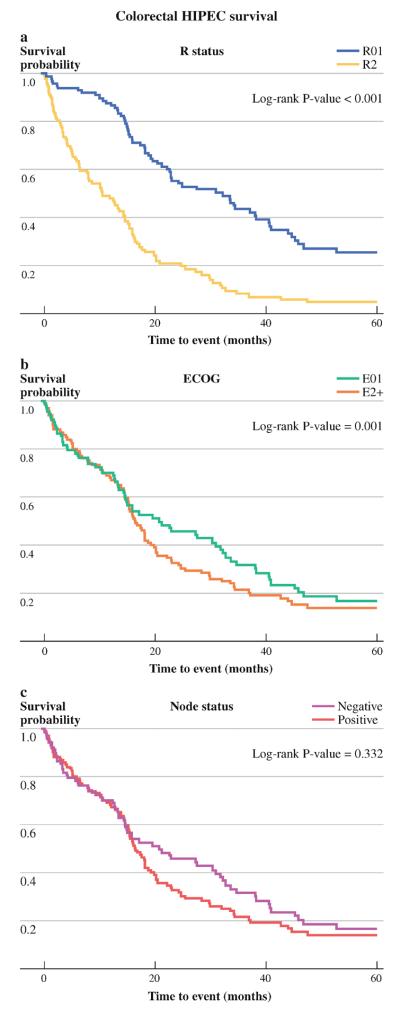
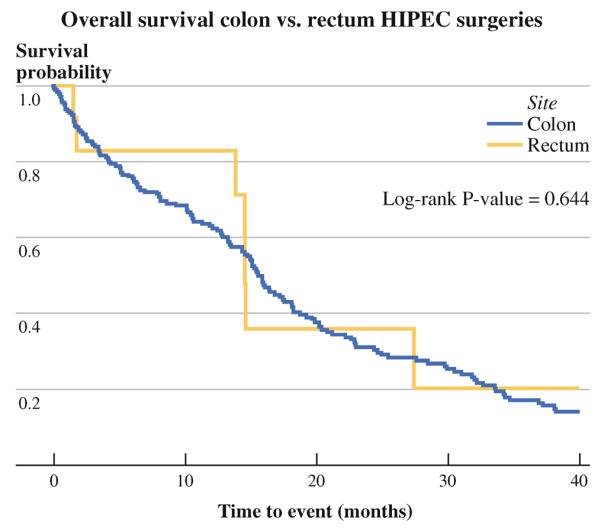
A total of 13 and 204 patients with PC from rectal and colon cancer, respectively, were identified. Median follow-up was 40.1 and 88.1 months, respectively. Eastern Cooperative Oncology Group (ECOG) score was zero or one for 92 % of patients with rectal cancer and 83 % for colon, while R1 resection was achieved in 54 and 51 %. The 30-day mortality was 5 % for colon cancer. There were no deaths in the rectal group. The morbidity for the colon and rectal groups was 57 and 46 %, respectively, with a 23 % 30-day readmission rate. In univariate analysis, age, ECOG, prior surgical score, albumin level, and node and resection status were not statistically significant in predicting survival for the rectal cancer patients. Median survival for the rectal and colon groups was 14.6 versus 17.3 months, while the 3-year survival was 28.2 versus 25.1 %.
Our data demonstrate similar 3-year survival for patients with rectal and colon cancer PC treated with CS/HIPEC. This can be attributed to patient selection bias. Selected rectal cancer PC patients should not be excluded from an attempted cytoreduction and HIPEC.
细胞减灭术(CS)联合腹腔热灌注化疗(HIPEC)是治疗腹膜癌(PC)最有可能延长生存时间的方法。然而,由于原发性肿瘤位于腹膜后,HIPEC 在直肠患者中的疗效存在争议。因此,我们回顾了我们在原发性直肠肿瘤患者中治疗 PC 的经验。
对 950 例 HIPEC 手术的前瞻性数据库进行回顾性分析。分析了患者的一般情况、年龄、白蛋白水平、既往手术评分、切除情况、发病率、死亡率和生存情况。
共发现直肠和结肠癌 PC 患者 13 例和 204 例,中位随访时间分别为 40.1 个月和 88.1 个月。直肠肿瘤患者中 ECOG 评分 0 或 1 的比例为 92%,结肠癌为 83%,R1 切除率为 54%和 51%。结肠癌的 30 天死亡率为 5%,直肠肿瘤组无死亡病例。结肠和直肠组的发病率分别为 57%和 46%,30 天再入院率为 23%。单因素分析显示,年龄、ECOG、既往手术评分、白蛋白水平以及淋巴结和切除情况对预测直肠肿瘤患者的生存均无统计学意义。直肠和结肠组的中位生存时间分别为 14.6 个月和 17.3 个月,3 年生存率分别为 28.2%和 25.1%。
我们的数据表明,接受 CS/HIPEC 治疗的直肠和结肠癌 PC 患者的 3 年生存率相似。这可以归因于患者选择偏倚。选择的直肠肿瘤 PC 患者不应被排除在尝试细胞减灭和 HIPEC 之外。