Division of Radiological and Imaging Sciences, University of Nottingham, Queen's Medical Campus, Nottingham, United Kingdom.
Ann Neurol. 2013 Jun;73(6):774-84. doi: 10.1002/ana.23876. Epub 2013 Jun 4.
There is a recognized need to improve selection of patients with carotid artery stenosis for carotid endarterectomy (CEA). We assessed the value of magnetic resonance imaging (MRI)-defined carotid plaque hemorrhage (MRIPH) to predict recurrent ipsilateral cerebral ischemic events, and stroke in symptomatic carotid stenosis.
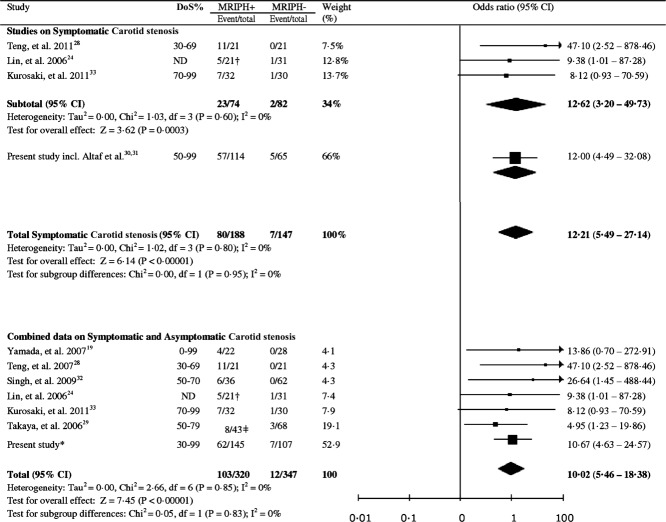
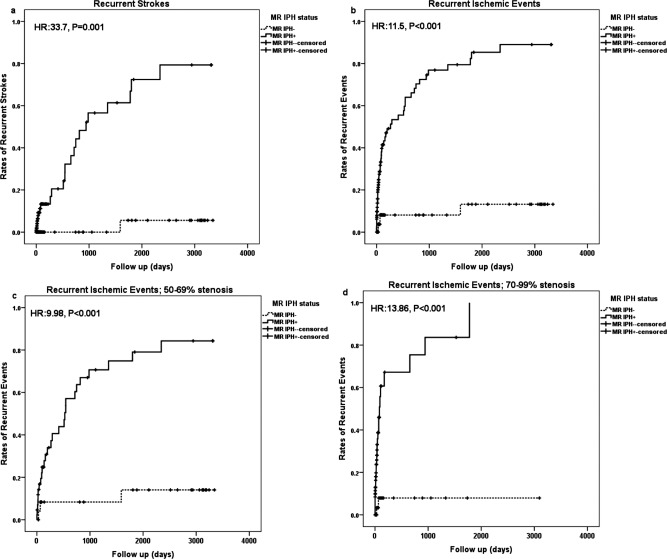
One hundred seventy-nine symptomatic patients with ≥ 50% stenosis were prospectively recruited, underwent carotid MRI, and were clinically followed up until CEA, death, or ischemic event. MRIPH was diagnosed if the plaque signal intensity was >150% that of the adjacent muscle. Event-free survival analysis was done using Kaplan-Meier plots and Cox regression models controlling for known vascular risk factors. We also undertook a meta-analysis of reported data on MRIPH and recurrent events.
One hundred fourteen patients (63.7%) showed MRIPH, suffering 92% (57 of 62) of all recurrent ipsilateral events and all but 1 (25 of 26) future strokes. Patients without MRIPH had an estimated annual absolute stroke risk of only 0.6%. Cox multivariate regression analysis proved MRIPH as a strong predictor of recurrent ischemic events (hazard ratio [HR] = 12.0, 95% confidence interval [CI] = 4.8-30.1, p < 0.001) and stroke alone (HR = 35.0, 95% CI = 4.7-261.6, p = 0.001). Meta-analysis of published data confirmed this association between MRIPH and recurrent cerebral ischemic events in symptomatic carotid artery stenosis (odds ratio = 12.2, 95% CI = 5.5-27.1, p < 0.00001).
MRIPH independently and strongly predicts recurrent ipsilateral ischemic events, and stroke alone, in symptomatic ≥ 50% carotid artery stenosis. The very low stroke risk in patients without MRIPH puts into question current risk-benefit assessment for CEA in this subgroup.
人们已经认识到需要改进颈动脉狭窄患者行颈动脉内膜切除术(CEA)的选择。我们评估了磁共振成像(MRI)定义的颈动脉斑块出血(MRIPH)对预测同侧复发性脑缺血事件和症状性颈动脉狭窄性卒中的价值。
前瞻性招募了 179 例≥50%狭窄的症状性患者,行颈动脉 MRI 检查,并进行临床随访,直至 CEA、死亡或发生缺血事件。如果斑块信号强度比相邻肌肉高 150%,则诊断为 MRIPH。采用 Kaplan-Meier 图和 Cox 回归模型进行无事件生存分析,控制已知血管危险因素。我们还对 MRIPH 与复发性事件的报告数据进行了荟萃分析。
114 例(63.7%)患者出现 MRIPH,发生了所有同侧复发性事件的 92%(57/62)和所有但 1 例(26/26)未来卒中。无 MRIPH 的患者估计每年的绝对卒中风险仅为 0.6%。Cox 多变量回归分析证明,MRIPH 是复发性缺血事件(危险比[HR] = 12.0,95%置信区间[CI] = 4.8-30.1,p < 0.001)和单独卒中的强烈预测因子(HR = 35.0,95% CI = 4.7-261.6,p = 0.001)。对已发表数据的荟萃分析证实了 MRIPH 与症状性颈动脉狭窄复发性脑缺血事件之间的这种关联(比值比= 12.2,95%CI = 5.5-27.1,p < 0.00001)。
MRIPH 可独立且强烈预测症状性≥50%颈动脉狭窄患者的同侧复发性缺血事件和单独卒中。无 MRIPH 的患者卒中风险极低,这对该亚组患者行 CEA 的风险效益评估提出了质疑。