Department of Pathology and Laboratory Medicine, Women & Infants Hospital, Alpert Medical School of Brown University, Providence, Rhode Island, USA.
Genet Med. 2013 Aug;15(8):600-11. doi: 10.1038/gim.2013.8. Epub 2013 Mar 14.
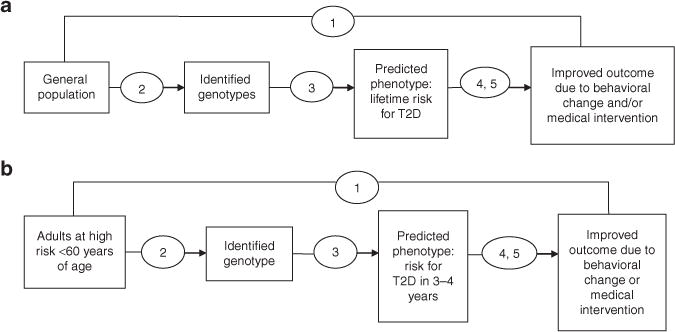
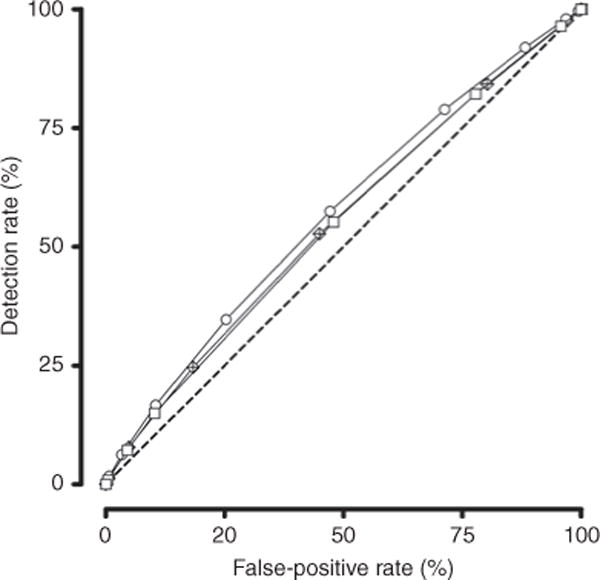
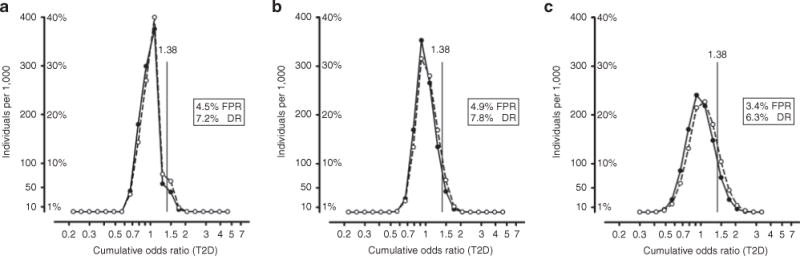
This evidence review addresses whether type 2 diabetes genomic risk panels improve health outcomes (e.g., reduce rates of developing type 2 diabetes) in low- or high-risk adults; two clinical scenarios promulgated by commercial companies offering such testing. Evidence for the analytic validity of available genomic profiles was inadequate. Clinical validity ranged from inadequate to convincing for 30 variants identified on five type 2 diabetes genomic panels and by genome-wide association studies. Eight common variants were identified for general population use; evidence credibility based on published criteria was strong for two variants, moderate for two variants, and weak for four variants. TCF7L2 had the largest per-allele odds ratio of 1.39 (95% confidence interval 1.33-1.46). Models combining the best four, best eight, and all 30 variants used summary effect sizes, reported genotype frequencies, and assumed independent effects. Areas under the curve were 0.547, 0.551, and 0.570, respectively. In high-risk populations, per-allele odds ratios for TCF7L2 alone were similar to those of the general population. TCF7L2, in combination with other variants, yielded minimal improvement in risk reclassification. Evidence on TCF7L2 clinical validity was adequate. Three studies addressed the clinical utility of intervention effectiveness, stratified by TCF7L2 genotype; none found significant interactions. Clinical utility evidence was inadequate. In addition to analytic validity and clinical utility knowledge gaps, additional gaps were identified regarding how to inform, produce, and evaluate models combining multiple variants.
本证据综述探讨了 2 型糖尿病基因组风险面板是否能改善低风险或高风险成年人的健康结果(例如,降低 2 型糖尿病的发病率);这是商业公司提供此类检测的两种临床情况。现有基因组谱的分析有效性证据不足。五种 2 型糖尿病基因组面板和全基因组关联研究确定的 30 个变体的临床有效性从不足到令人信服不等。确定了八种常见变体可用于一般人群;根据已发布标准,两种变体的证据可信度较强,两种变体的证据可信度中等,四种变体的证据可信度较弱。TCF7L2 的等位基因比值比最大,为 1.39(95%置信区间 1.33-1.46)。结合最佳四个、最佳八个和所有 30 个变体的模型使用了汇总效应大小、报告的基因型频率,并假设了独立效应。曲线下面积分别为 0.547、0.551 和 0.570。在高危人群中,TCF7L2 单一等位基因的比值比与一般人群相似。TCF7L2 与其他变体结合使用,对风险再分类的改善作用很小。TCF7L2 临床有效性的证据是充分的。有三项研究根据 TCF7L2 基因型探讨了干预效果的临床实用性;均未发现显著的交互作用。临床实用性证据不足。除了分析有效性和临床实用性知识差距外,还确定了如何告知、产生和评估结合多个变体的模型的其他差距。