Department of Infection, Barts Health NHS Trust, Royal London Hospital, London E1 2ES, UK.
Postgrad Med J. 2013 Jun;89(1052):329-34. doi: 10.1136/postgradmedj-2012-131393. Epub 2013 Mar 21.
There is lack of contemporary outcome data on patients with hospital-acquired infections that cause bacteraemia. We determined the risk factors for 7-day mortality and investigated the hypothesis that, compared with central venous catheter (CVC)-associated bacteraemic infections, catheter-associated bacteraemic urinary tract infections (UTIs) were significantly associated with 7-day mortality.
From October 2007 to September 2008, demographical, clinical and microbiological data were collected on patients with hospital-acquired bacteraemia. Patients were followed until death, hospital discharge or recovery from infection. Risk factors for 7-day mortality were determined and multivariate logistic regression was used to define the association between catheter-associated bacteraemic UTIs and likelihood of death.
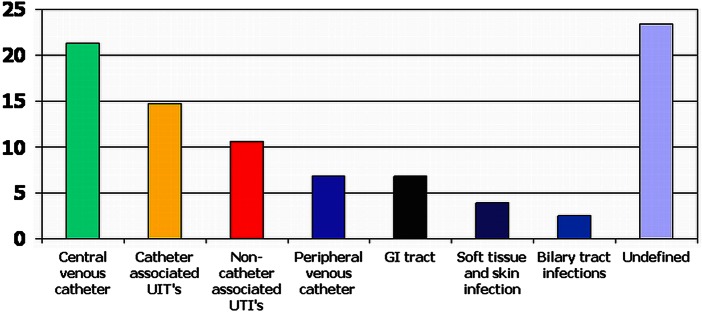
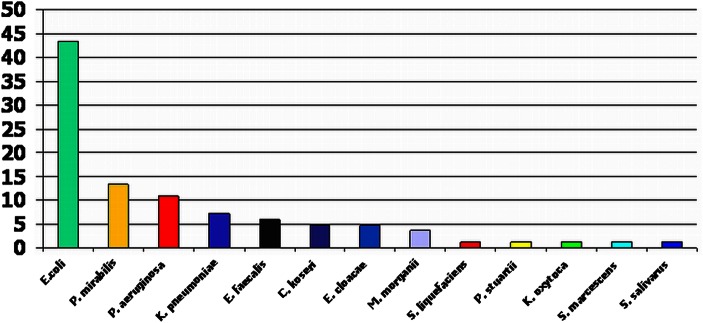
559 bacteraemic episodes occurred in 437 patients. Overall, there were 90 deaths (20.6%) at 7 days and 153 deaths (35.0%) at 30 days. Among patients with catheter-associated bacteraemic UTIs, 7-day and 30-day mortalities associated with each bacteraemic episode were 25/83 (30.1%) and 33/83 (39.8%), respectively. Within this subgroup, the commonest isolates were Escherichia coli, 36 (43.4%), Proteus mirabilis, 11 (13.3%) and Pseudomonas aeruginosa, 9 (10.8%). There were 22 (26.5%) multiple drug-resistant isolates and, of the E coli infections, 6 (16.7%) were extended spectrum β-lactamase producers. In univariate analysis, the variables found to have the strongest association with 7-day mortality were age, Pitt score, Charlson comorbidity index (CCI), medical speciality and site of infection. Compared with CVC-associated bacteraemic infections, there was a significant association between catheter-associated bacteraemic UTIs and 7-day mortality (OR 4.16, 95% CI 1.86 to 9.33). After adjustment for age and CCI, this association remained significant (OR 2.90, 95% CI 1.19 to 7.07).
Compared with CVC-associated bacteraemic infections, catheter-associated bacteraemic UTIs were significantly associated with 7-day mortality. Efforts to reduce these infections should be prioritised.
目前缺乏有关医院获得性感染导致菌血症患者的当代结局数据。我们确定了 7 天死亡率的危险因素,并研究了以下假设,即与中心静脉导管(CVC)相关的菌血症感染相比,导管相关菌血症尿路感染(UTI)与 7 天死亡率显著相关。
2007 年 10 月至 2008 年 9 月,收集了医院获得性菌血症患者的人口统计学、临床和微生物学数据。患者随访至死亡、出院或感染痊愈。确定了 7 天死亡率的危险因素,并使用多变量逻辑回归来定义导管相关菌血症 UTI 与死亡可能性之间的关联。
437 例患者发生 559 例菌血症发作。总体而言,7 天时有 90 例(20.6%)死亡,30 天时有 153 例(35.0%)死亡。在导管相关菌血症 UTI 患者中,每个菌血症发作的 7 天和 30 天死亡率分别为 25/83(30.1%)和 33/83(39.8%)。在这一分组中,最常见的分离株是大肠埃希菌,36 株(43.4%),奇异变形杆菌 11 株(13.3%)和铜绿假单胞菌 9 株(10.8%)。有 22 株(26.5%)为多重耐药株,在大肠埃希菌感染中,有 6 株(16.7%)为产超广谱β-内酰胺酶株。在单变量分析中,与 7 天死亡率相关性最强的变量是年龄、Pitt 评分、Charlson 合并症指数(CCI)、医学专业和感染部位。与 CVC 相关的菌血症感染相比,导管相关菌血症 UTI 与 7 天死亡率显著相关(OR 4.16,95%CI 1.86 至 9.33)。在调整年龄和 CCI 后,这种关联仍然显著(OR 2.90,95%CI 1.19 至 7.07)。
与 CVC 相关的菌血症感染相比,导管相关菌血症 UTI 与 7 天死亡率显著相关。应优先努力减少这些感染。