Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Am J Kidney Dis. 2013 Aug;62(2):245-52. doi: 10.1053/j.ajkd.2013.03.009. Epub 2013 Apr 6.
Lifetime risk estimates of chronic kidney disease (CKD) can motivate preventative behaviors at the individual level and forecast disease burden and health care use at the population level.
Markov Monte Carlo model simulation study.
SETTING & POPULATION: Current US black and white population.
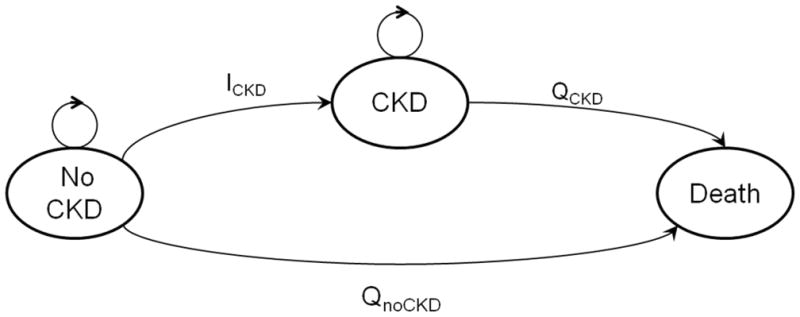
MODEL, PERSPECTIVE, & TIMEFRAME: Markov models simulating kidney disease development, using an individual perspective and lifetime horizon.
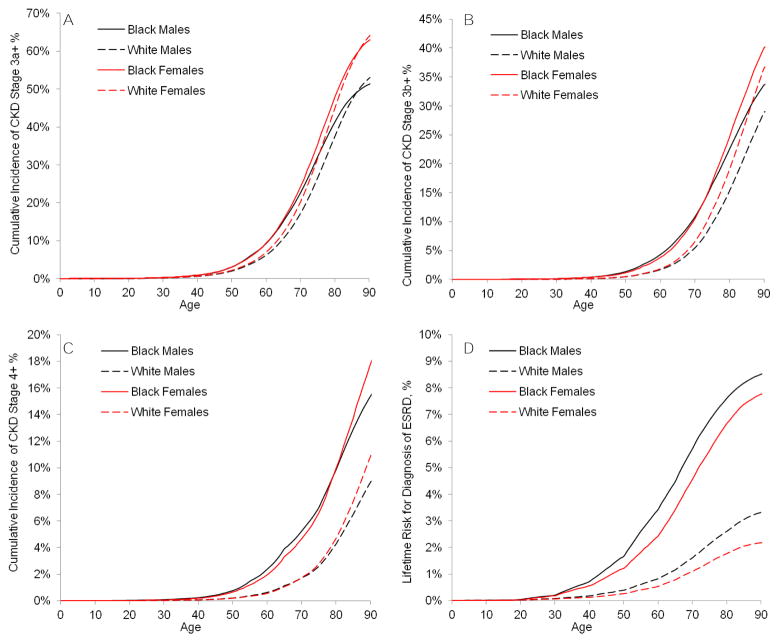
Age-, sex-, and race-specific residual lifetime risks of CKD stages 3a+ (estimated glomerular filtration rate [eGFR] <60 mL/min/1.73 m²), 3b+ (eGFR <45 mL/min/1.73 m²), 4+ (eGFR <30 mL/min/1.73 m²), and end-stage renal disease (ESRD).
State transition probabilities of developing CKD and of dying prior to its development were modeled using: (1) mortality rates from the National Vital Statistics Report, (2) mortality risk estimates from a 2-million person meta-analysis, and (3) CKD prevalence from National Health and Nutrition Examination Surveys. Incidence, prevalence, and mortality related to ESRD were supplied by the US Renal Data System.
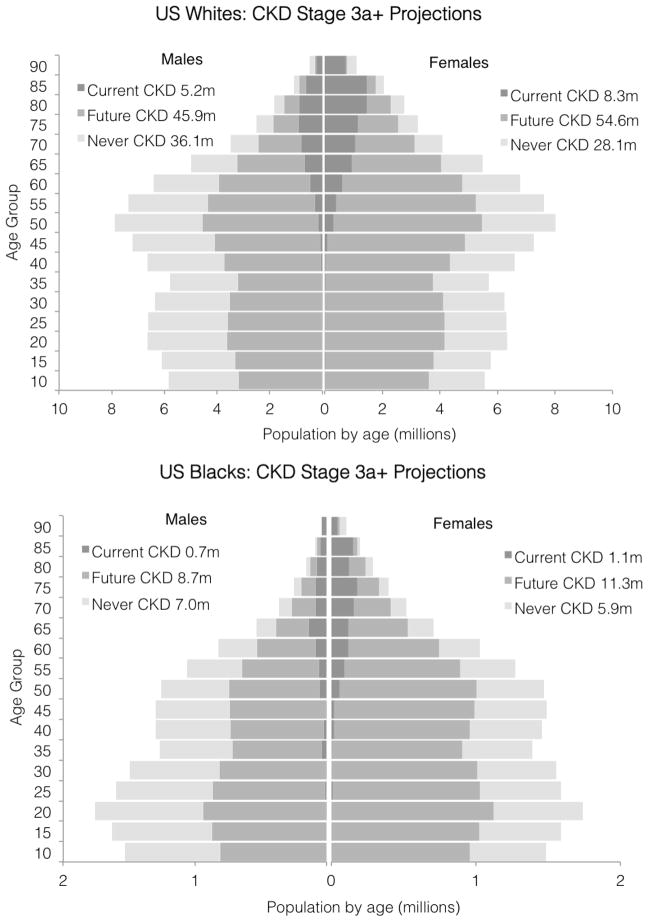
At birth, the overall lifetime risks of CKD stages 3a+, 3b+, 4+, and ESRD were 59.1%, 33.6%, 11.5%, and 3.6%, respectively. Women experienced greater CKD risk yet lower ESRD risk than men; blacks of both sexes had markedly higher CKD stage 4+ and ESRD risks (lifetime risks for white men, white women, black men, and black women, respectively: CKD stage 3a+, 53.6%, 64.9%, 51.8%, and 63.6%; CKD stage 3b+, 29.0%, 36.7%, 33.7%, and 40.2%; CKD stage 4+, 9.3%, 11.4%, 15.8%, and 18.5%; and ESRD, 3.3%, 2.2%, 8.5%, and 7.8%). Risk of CKD increased with age, with approximately one-half the CKD stage 3a+ cases developing after 70 years of age.
CKD incidence was modeled from prevalence estimates in the US population.
In the United States, the lifetime risk of developing CKD stage 3a+ is high, emphasizing the importance of primary prevention and effective therapy to reduce CKD-related morbidity and mortality.
慢性肾脏病 (CKD) 的终生风险估计可以在个体层面激发预防行为,并预测人群层面的疾病负担和医疗保健使用。
马尔可夫蒙特卡罗模型模拟研究。
当前美国的黑人和白人。
模型、观点和时间范围:使用个体视角和终生范围模拟肾脏疾病发展的马尔可夫模型。
年龄、性别和种族特异性 CKD 阶段 3a+(估计肾小球滤过率[eGFR]<60 mL/min/1.73 m²)、3b+(eGFR<45 mL/min/1.73 m²)、4+(eGFR<30 mL/min/1.73 m²)和终末期肾病(ESRD)的残余终生风险。
使用以下方法对发展 CKD 和在其发展之前死亡的状态转移概率进行建模:(1)来自国家生命统计报告的死亡率,(2)来自 200 万人荟萃分析的死亡率风险估计,以及(3)来自国家健康和营养检查调查的 CKD 患病率。ESRD 相关的发病率、患病率和死亡率由美国肾脏数据系统提供。
出生时,CKD 阶段 3a+、3b+、4+和 ESRD 的总体终生风险分别为 59.1%、33.6%、11.5%和 3.6%。女性经历的 CKD 风险高于男性,但 ESRD 风险低于男性;黑人性别都有明显更高的 CKD 阶段 4+和 ESRD 风险(白人男性、白人女性、黑人男性和黑人女性的终生风险分别为:CKD 阶段 3a+,53.6%、64.9%、51.8%和 63.6%;CKD 阶段 3b+,29.0%、36.7%、33.7%和 40.2%;CKD 阶段 4+,9.3%、11.4%、15.8%和 18.5%;和 ESRD,3.3%、2.2%、8.5%和 7.8%)。CKD 风险随年龄增长而增加,大约一半的 CKD 阶段 3a+病例发生在 70 岁以后。
CKD 发病率是根据美国人口的患病率估计模型化的。
在美国,发展 CKD 阶段 3a+的终生风险很高,这强调了初级预防和有效治疗的重要性,以降低与 CKD 相关的发病率和死亡率。