Division of Cardiology, University of Washington, Seattle, WA 98195, USA.
AJR Am J Roentgenol. 2013 May;200(5):W450-7. doi: 10.2214/AJR.12.8934.
Coronary CT angiography has high sensitivity, but modest specificity, to detect acute coronary syndrome. We studied whether adding resting CT myocardial perfusion imaging improved the detection of acute coronary syndrome.
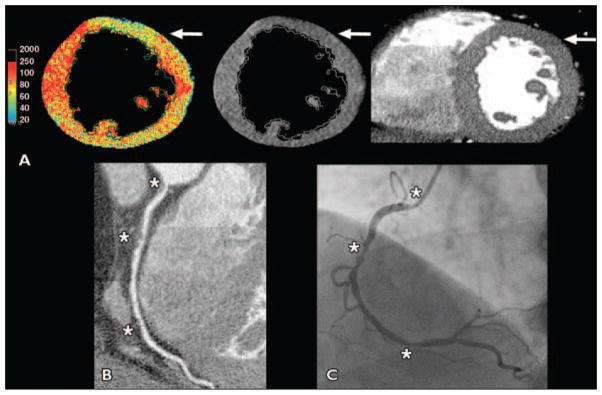
Patients with low-to-intermediate cardiac risk presenting with possible acute coronary syndrome received both the standard of care evaluation and a research thoracic 64-MDCT examination. Patients with an obstructive (> 50%) stenosis or a nonevaluable coronary segment on CT were diagnosed with possible acute coronary syndrome. CT perfusion was determined by applying gray and color Hounsfield unit maps to resting CT angiography images. Adjudicated patient diagnoses were based on the standard of care and 3-month follow-up. Patient-level diagnostic performance for acute coronary syndrome was calculated for coronary CT, CT perfusion, and combined techniques.
A total of 105 patients were enrolled. Of the nine (9%) patients with acute coronary syndrome, all had obstructive CT stenoses but only three had abnormal CT perfusion. CT perfusion was normal in all other patients. To detect acute coronary syndrome, CT angiography had 100% sensitivity, 89% specificity, and a positive predictive value of 45%. For CT perfusion, specificity and positive predictive value were each 100%, and sensitivity was 33%. Combined cardiac CT and CT perfusion had similar specificity but a higher positive predictive value (100%) than did CT angiography.
Resting CT perfusion using CT angiographic images may have high specificity and may improve CT positive predictive value for acute coronary syndrome without added radiation and contrast. However, normal resting CT perfusion cannot exclude acute coronary syndrome.
冠状动脉 CT 血管造影术对检测急性冠状动脉综合征具有较高的敏感性,但特异性较低。我们研究了静息 CT 心肌灌注成像是否能提高急性冠状动脉综合征的检出率。
低至中度心脏风险的患者出现可能的急性冠状动脉综合征时,接受标准护理评估和研究性胸部 64-MDCT 检查。CT 上有>50%的阻塞性狭窄或无法评估的冠状动脉节段的患者被诊断为可能的急性冠状动脉综合征。通过将灰度和彩色亨氏单位图应用于静息 CT 血管造影图像来确定 CT 灌注。经裁决的患者诊断结果基于标准护理和 3 个月的随访。计算冠状动脉 CT、CT 灌注和联合技术对急性冠状动脉综合征的患者水平诊断性能。
共纳入 105 例患者。在 9%(9 例)的急性冠状动脉综合征患者中,所有患者均有阻塞性 CT 狭窄,但只有 3 例有异常 CT 灌注。所有其他患者的 CT 灌注均正常。为了检测急性冠状动脉综合征,CT 血管造影术的敏感性为 100%,特异性为 89%,阳性预测值为 45%。对于 CT 灌注,特异性和阳性预测值均为 100%,而敏感性为 33%。与 CT 血管造影术相比,联合心脏 CT 和 CT 灌注的特异性相似,但阳性预测值更高(100%)。
使用 CT 血管造影图像的静息 CT 灌注可能具有较高的特异性,并可能提高 CT 对急性冠状动脉综合征的阳性预测值,而不会增加辐射和对比剂的使用。然而,正常的静息 CT 灌注并不能排除急性冠状动脉综合征。