Department of Pharmacology, University of Alberta, Edmonton, Canada.
PLoS One. 2013 Apr 23;8(4):e62349. doi: 10.1371/journal.pone.0062349. Print 2013.
To investigate the use of liposomal irinotecan (Irinophore C™) plus or minus 5-fluorouracil (5-FU) for the treatment of colorectal cancer.
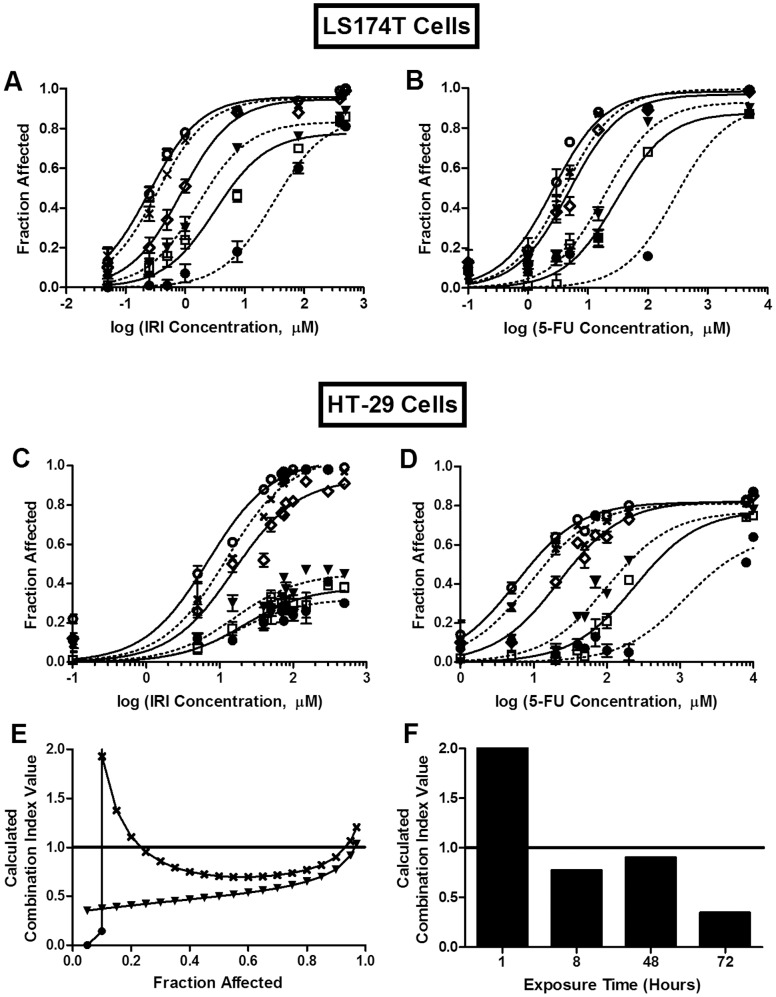
The effect of irinotecan (IRI) and/or 5-FU exposure times on cytotoxicity was assessed in vitro against HT-29 or LS174T human colon carcinoma cells. The pharmacokinetics and biodistribution of Irinophore C™ (IrC™) and 5-FU, administered alone or in combination, were compared in vivo. A subcutaneous model of HT-29 human colorectal cancer in Rag2-M mice was utilized to assess the efficacy of IrC™ alone, and in combination with 5-FU.
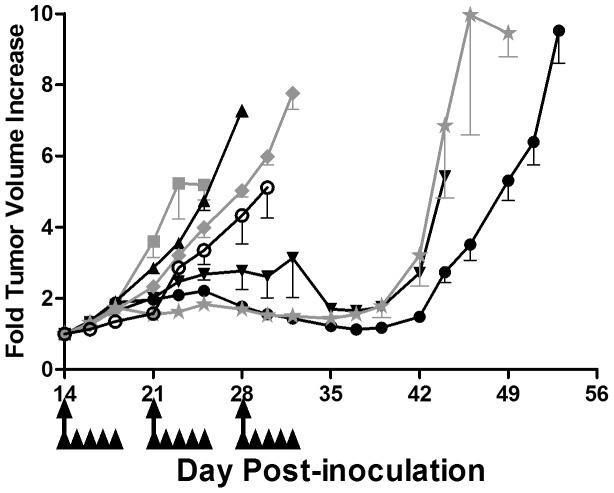
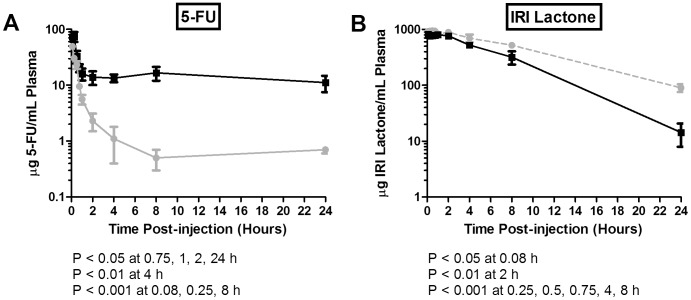
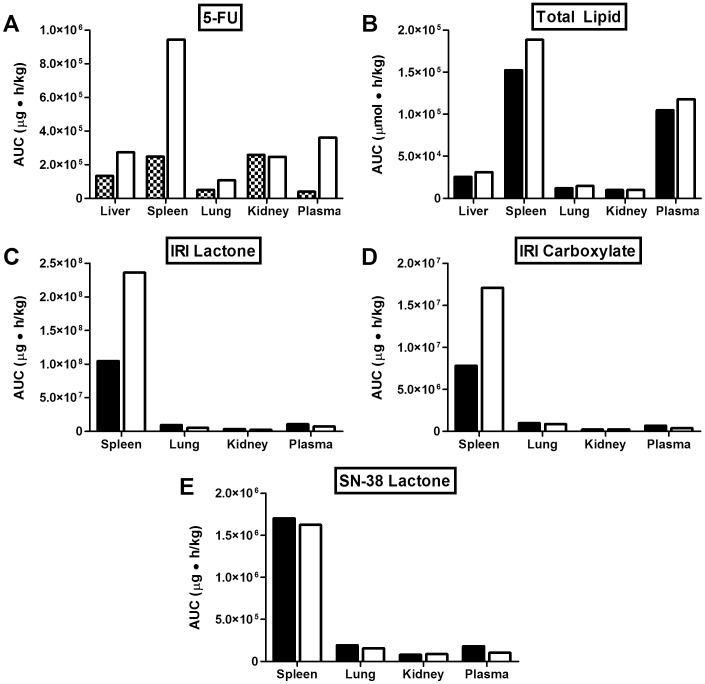
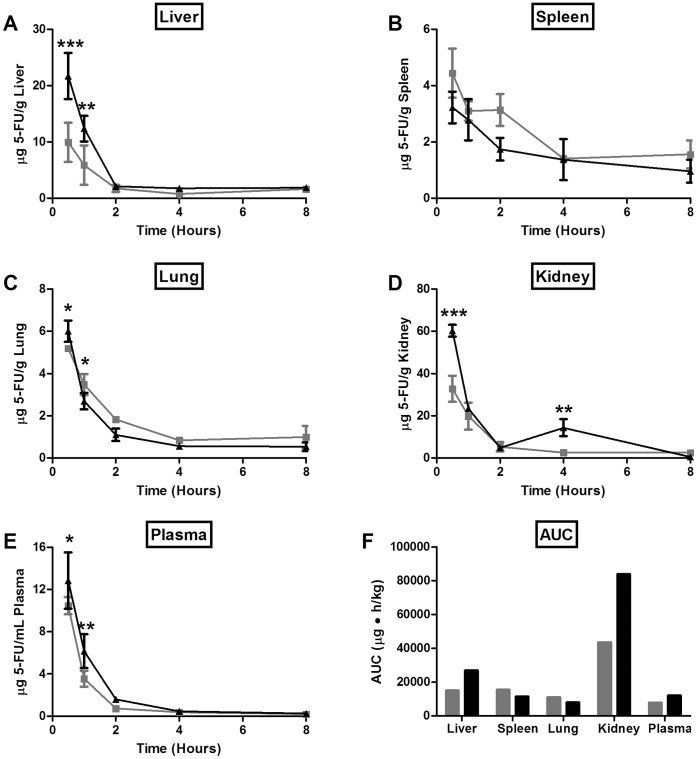
The cytotoxicity of IRI and 5-FU were strongly dependent on exposure time. Synergistic interactions were observed following prolonged exposure to IRI/5-FU combinations. Pharmacokinetics/biodistribution studies demonstrated that the 5-FU elimination rate was decreased significantly when 5-FU was co-administered intravenously with IrC™, versus alone. Significant decreases in 5-FU elimination were also observed in plasma, with an associated increase of 5-FU in some tissues when 5-FU was given by intraperitoneal injection and IrC™ was given intravenously. The elimination of IrC™ was not significantly different when administered alone or in combination with 5-FU. Therapeutic studies demonstrated that single agent IrC™ was significantly more effective than the combination of IRI/5-FU; surprisingly, IrC™/5-FU combinations were no more effective than IrC™ alone. The administration of combinations of 5-FU (16 mg/kg) and IrC™ (60 mg IRI/kg) showed increased toxicity when compared to IrC™ alone. Treatment with IrC™ alone (60 mg IRI/kg) delayed the time required for a 5-fold increase in initial tumor volume to day 49, compared to day 23 for controls. When IrC™ (40 mg IRI/kg) was used in combination with 5-FU (16 mg/kg), the time to increase tumor volume 5-fold was 43 days, which was comparable to that achieved when using IrC™ alone (40 mg IRI/kg).
Single agent IrC™ was well tolerated and has significant therapeutic potential. IrC™ may be a suitable replacement for IRI treatment, but its use with free 5-FU is complicated by IrC™-engendered changes in 5-FU pharmacokinetics/biodistribution which are associated with increased toxicity when using the combination.
研究脂质体伊立替康(Irinophore C™)联合或不联合 5-氟尿嘧啶(5-FU)治疗结直肠癌。
评估伊立替康(IRI)和/或 5-FU 暴露时间对 HT-29 或 LS174T 人结肠癌细胞的体外细胞毒性。体内比较 Irinophore C™(IrC™)和 5-FU 单独或联合给药的药代动力学和生物分布。利用 Rag2-M 小鼠皮下 HT-29 人结直肠癌细胞模型评估 IrC™单独使用以及与 5-FU 联合使用的疗效。
IRI 和 5-FU 的细胞毒性强烈依赖于暴露时间。长时间联合应用 IRI/5-FU 可观察到协同作用。药代动力学/生物分布研究表明,与单独静脉注射 5-FU 相比,5-FU 与 IrC™ 同时静脉注射时,5-FU 的消除率显著降低。当腹腔注射 5-FU 和静脉注射 IrC™ 时,5-FU 在血浆中的消除也明显减少,同时一些组织中 5-FU 增加。当单独给予 IrC™ 或与 5-FU 联合给予时,IrC™ 的消除没有显著差异。治疗研究表明,单一药物 IrC™ 比 IRI/5-FU 联合治疗更有效;令人惊讶的是,IrC™/5-FU 联合治疗并不比 IrC™ 单独治疗更有效。与单独使用 IrC™ 相比,5-FU(16 mg/kg)和 IrC™(60 mg IRI/kg)联合使用的组合显示出增加的毒性。单独使用 IrC™(60 mg IRI/kg)可将初始肿瘤体积增加 5 倍所需的时间延迟至第 49 天,而对照组为第 23 天。当 IrC™(40 mg IRI/kg)与 5-FU(16 mg/kg)联合使用时,肿瘤体积增加 5 倍所需的时间为 43 天,与单独使用 IrC™(40 mg IRI/kg)相当。
单一药物 IrC™ 耐受性良好,具有显著的治疗潜力。IrC™ 可能是 IRI 治疗的合适替代品,但由于 IrC™ 引起的 5-FU 药代动力学/生物分布变化,当联合使用时会增加毒性,因此其与游离 5-FU 的联合使用较为复杂。