Department of Public Health, Erasmus Medical Center, P.O. Box 2040, Rotterdam, 3000, CA, The Netherlands.
Br J Cancer. 2013 May 28;108(10):1971-7. doi: 10.1038/bjc.2013.198. Epub 2013 May 14.
Men with screen-detected prostate cancer can choose to undergo immediate curative treatment or enter into an expectant management programme. We quantified how the benefits and harms of immediate treatment vary according to the prognostic factors of clinical T-stage, Gleason score, and patient age.
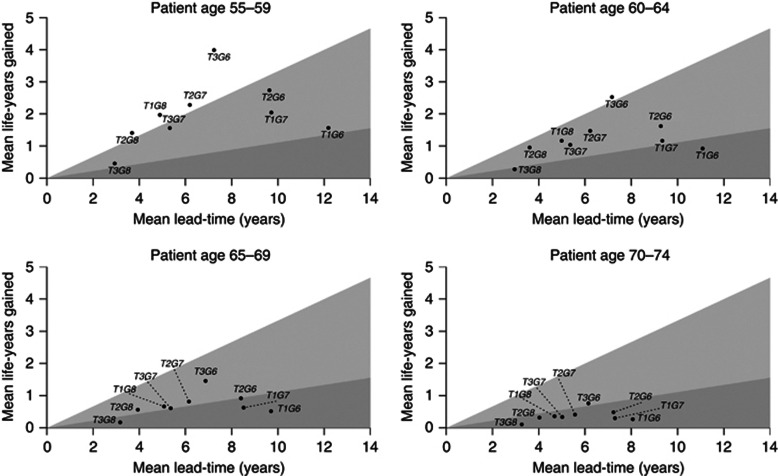
A microsimulation model based on European Randomized Study of Screening for Prostate Cancer data was used to predict the benefits and harms of immediate treatment versus delayed treatment of local-regional prostate cancer in men aged 55-74 years. Benefits included life-years gained and reduced probability of death from prostate cancer. Harms included lead time and probability of overdiagnosis.
The ratio of mean lead time to mean life-years gained ranged from 1.8 to 31.2, and the additional number of treatments required per prostate cancer death prevented ranged from 0.3 to 11.6 across the different prognostic groups. Both harm-benefit ratios were lowest, most favourable, for men aged 55-59 years and diagnosed with moderate-risk prostate cancer. Ratios were high for men aged 70-74 years regardless of clinical T-stage and Gleason score.
Men aged 55-59 years with moderate-risk prostate cancer are predicted to derive greatest benefit from immediate curative treatment. Immediate treatment is least favourable for men aged 70-74 years with either low-risk or high-risk prostate cancer.
通过屏幕检测出患有前列腺癌的男性可以选择接受立即治愈性治疗或进入期待管理方案。我们量化了立即治疗的益处和危害如何根据临床 T 期、Gleason 评分和患者年龄的预后因素而变化。
使用基于欧洲前列腺癌筛查随机研究数据的微模拟模型来预测 55-74 岁男性局部区域性前列腺癌的立即治疗与延迟治疗的益处和危害。益处包括获得的寿命年数和降低死于前列腺癌的概率。危害包括领先时间和过度诊断的概率。
不同预后组的平均领先时间与平均寿命年数增益之比范围为 1.8 至 31.2,每预防一例前列腺癌死亡所需的额外治疗次数范围为 0.3 至 11.6。对于年龄在 55-59 岁且诊断为中度风险前列腺癌的男性,这两个危害-效益比均最低,最有利。无论临床 T 期和 Gleason 评分如何,年龄在 70-74 岁的男性的比值均较高。
预计年龄在 55-59 岁且患有中度风险前列腺癌的男性将从立即治愈性治疗中获得最大益处。对于年龄在 70-74 岁且患有低危或高危前列腺癌的男性,立即治疗最不利。