Department of Gynecology and Obstetrics, University of Regensburg, Caritas Krankenhaus St. Josef Regensburg, Landshuter Straße 65, 93053, Regensburg, Germany.
Breast Cancer Res Treat. 2013 Jun;139(2):539-52. doi: 10.1007/s10549-013-2560-8. Epub 2013 May 16.
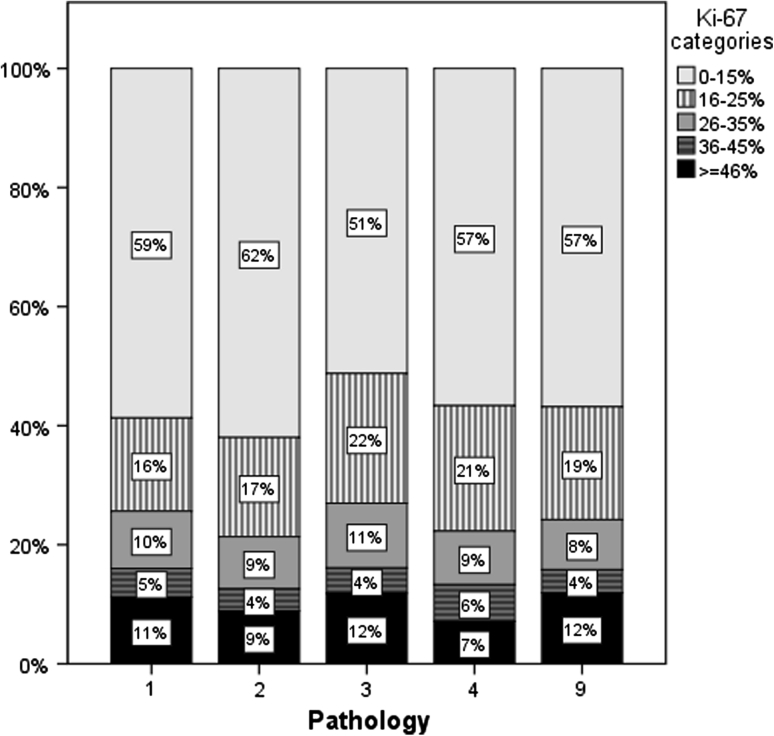
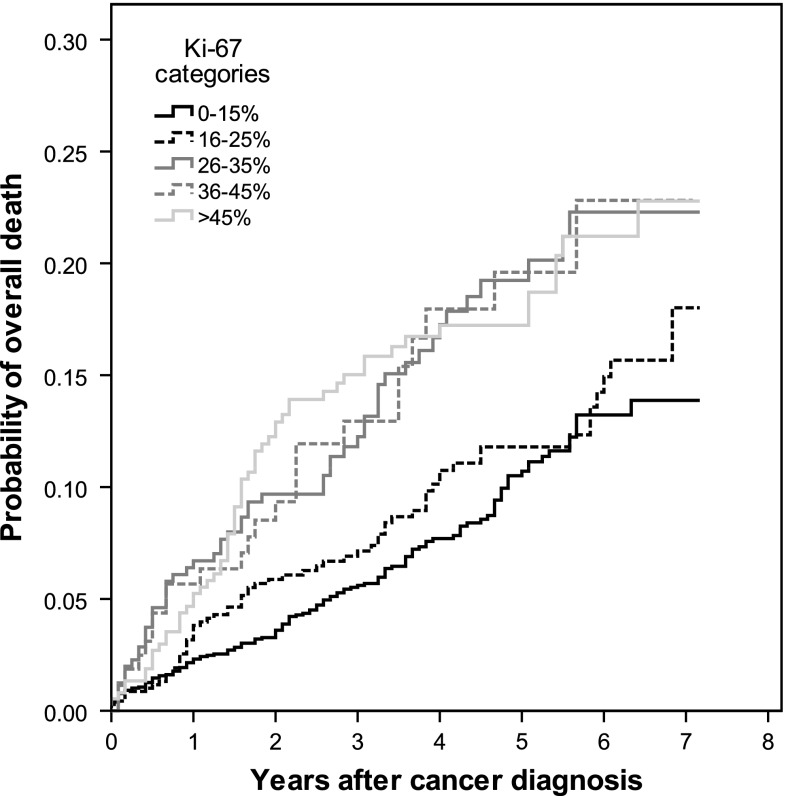
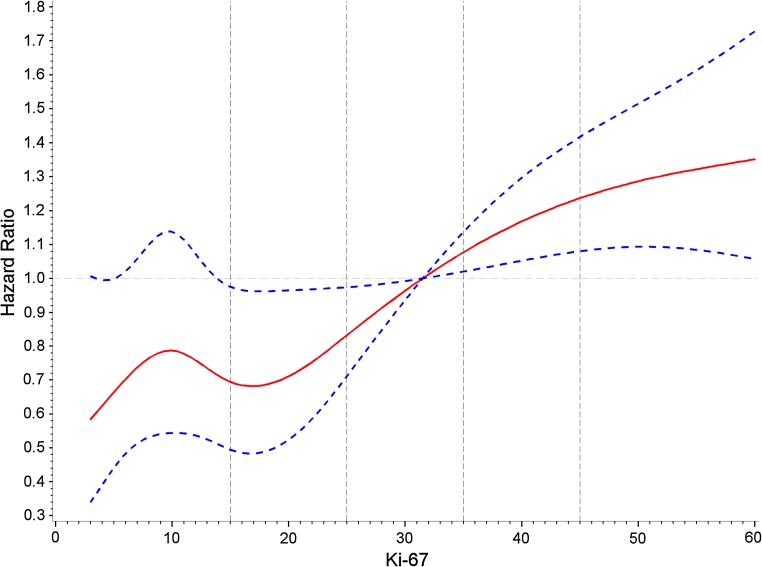
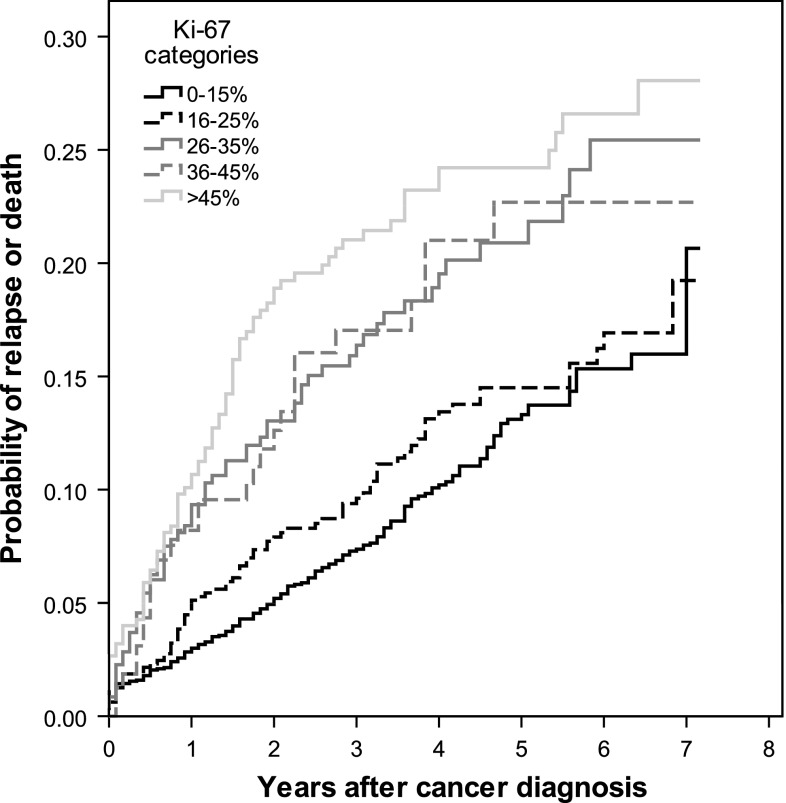
The proliferation marker Ki-67 is one of the most controversially discussed parameters for treatment decisions in breast cancer patients. The purpose of this study was to evaluate the routine use and value of Ki-67 as a prognostic marker, and to analyze the associations between Ki-67 and common histopathological parameters in the routine clinical setting. Data from the clinical cancer registry Regensburg (Bavaria, Germany) were analyzed. Within the total data pool of 4,692 female patients, who had been diagnosed between 2005 and 2011, in 3,658 cases Ki-67 was routinely determined. Thus, a total of 3,658 patients with invasive breast cancer were included in the present study and used for statistical analysis. Ki-67 expression was associated with the common histopathological parameters. The strongest correlation was found between grading and Ki-67 (P < 0.001). In terms of survival analyses, Ki-67 was categorized into five categories (reference category Ki-67 ≤15 %) due to a nonlinear relationship to overall survival (OS). In multivariable analysis, Ki-67 was an independent prognostic parameter both for disease-free survival (DFS) (Ki-67 > 45 %, HR = 1.96, P = 0.001) as well as for OS (Ki-67: 26-35 %, HR = 1.71, P = 0.017; Ki-67: 36-45 %, HR = 2.05, P = 0.011; Ki-67 > 45 %, HR = 2.06, P = 0.002) independent of common clinical and histopathological factors. The 5-year DFS (OS) rate was 86.7 % (89.3 %) in patients with a Ki-67 value ≤15 % compared to 75.8 % (82.8 %) in patients with a Ki-67 value >45 %. Based on the data from a large cohort of a clinical cancer registry, it was demonstrated that Ki-67 is frequently determined in routine clinical work. Ki-67 expression is associated with common histopathological parameters, but is an additional independent prognostic parameter for DFS and OS in breast cancer patients. Future work should focus on standardization of Ki-67 assessment and specification of its role in treatment decisions.
增殖标志物 Ki-67 是乳腺癌患者治疗决策中最具争议的参数之一。本研究旨在评估 Ki-67 作为预后标志物的常规使用和价值,并分析 Ki-67 与常规临床环境中常见组织病理学参数之间的关联。分析了来自德国巴伐利亚雷根斯堡临床癌症登记处的数据。在 2005 年至 2011 年间诊断的 4692 名女性患者的总数据集中,有 3658 例患者常规测定 Ki-67。因此,本研究共纳入 3658 例浸润性乳腺癌患者,并进行了统计学分析。Ki-67 表达与常见组织病理学参数相关。分级与 Ki-67 之间的相关性最强(P<0.001)。在生存分析方面,由于 Ki-67 与总生存期(OS)之间呈非线性关系,因此 Ki-67 分为五个类别(参考类别 Ki-67≤15%)。在多变量分析中,Ki-67 是无病生存期(DFS)(Ki-67>45%,HR=1.96,P=0.001)和 OS(Ki-67:26-35%,HR=1.71,P=0.017;Ki-67:36-45%,HR=2.05,P=0.011;Ki-67>45%,HR=2.06,P=0.002)的独立预后参数,独立于常见的临床和组织病理学因素。Ki-67 值≤15%的患者 5 年 DFS(OS)率为 86.7%(89.3%),而 Ki-67 值>45%的患者为 75.8%(82.8%)。基于临床癌症登记处的大型队列数据,本研究表明 Ki-67 在常规临床工作中经常被测定。Ki-67 的表达与常见的组织病理学参数相关,但在乳腺癌患者的 DFS 和 OS 中是一个额外的独立预后参数。未来的工作应集中在 Ki-67 评估的标准化和明确其在治疗决策中的作用。