Division of Neurology, Department of Pediatrics, Cincinnati Children's Hospital Medical Center Cincinnati, OH, USA.
Front Neurol. 2013 May 14;4:56. doi: 10.3389/fneur.2013.00056. eCollection 2013.
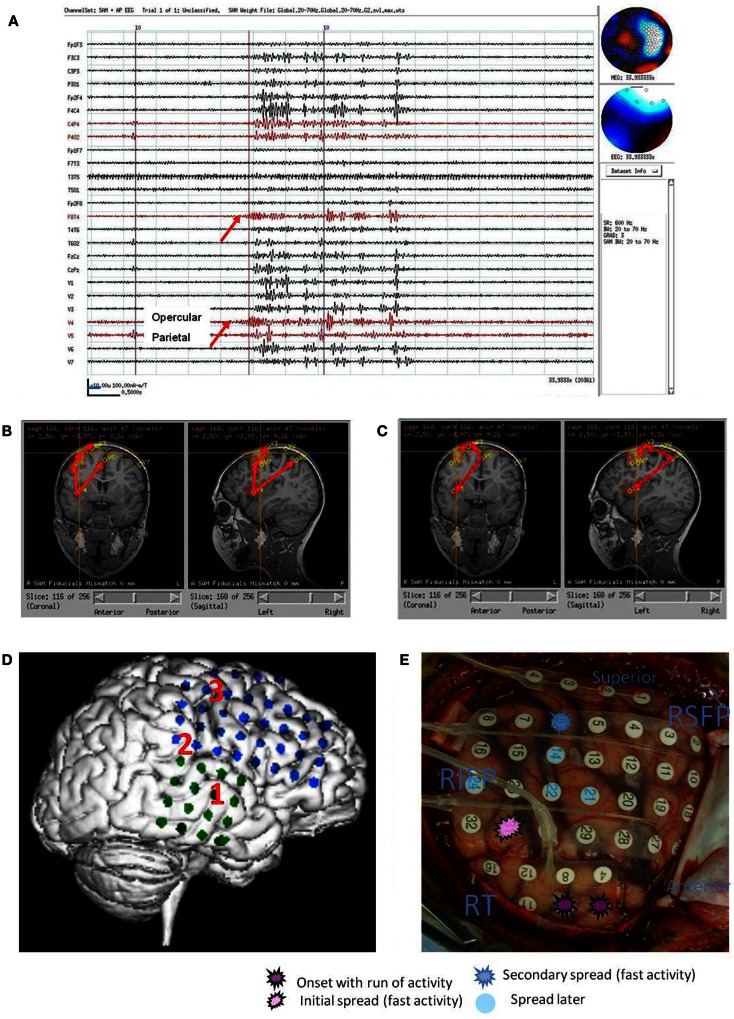
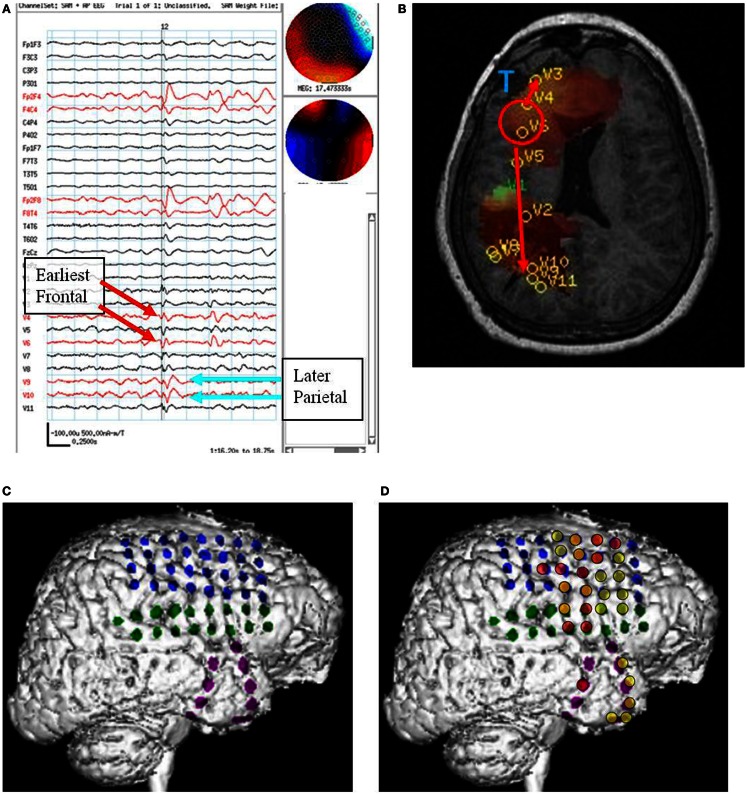
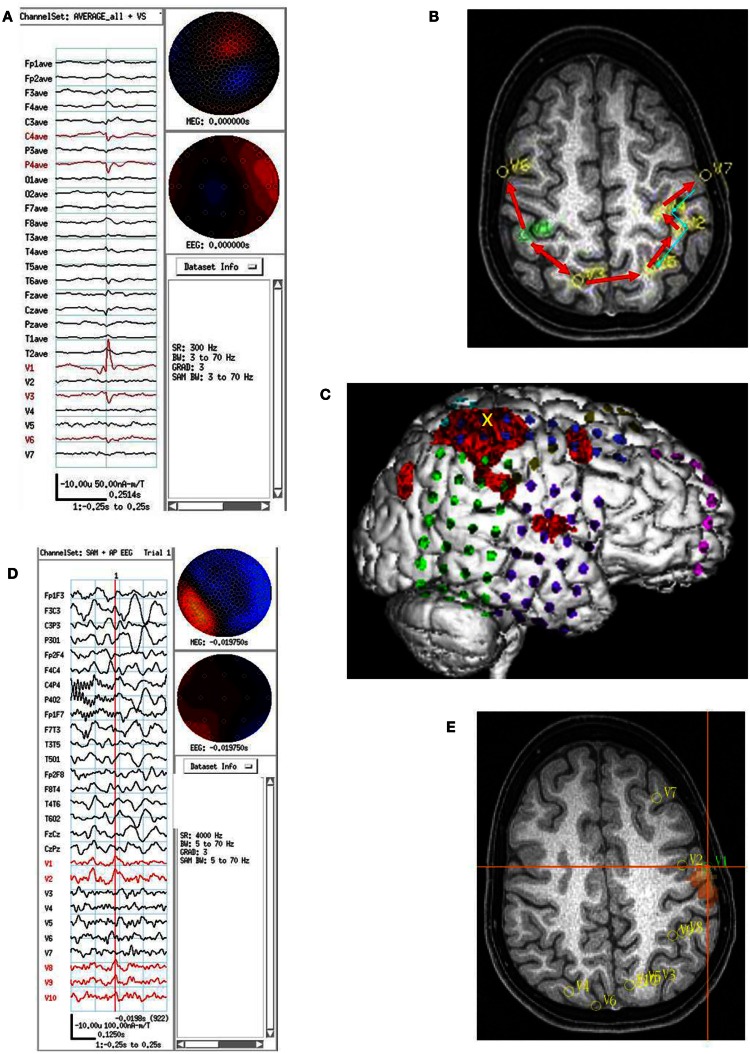
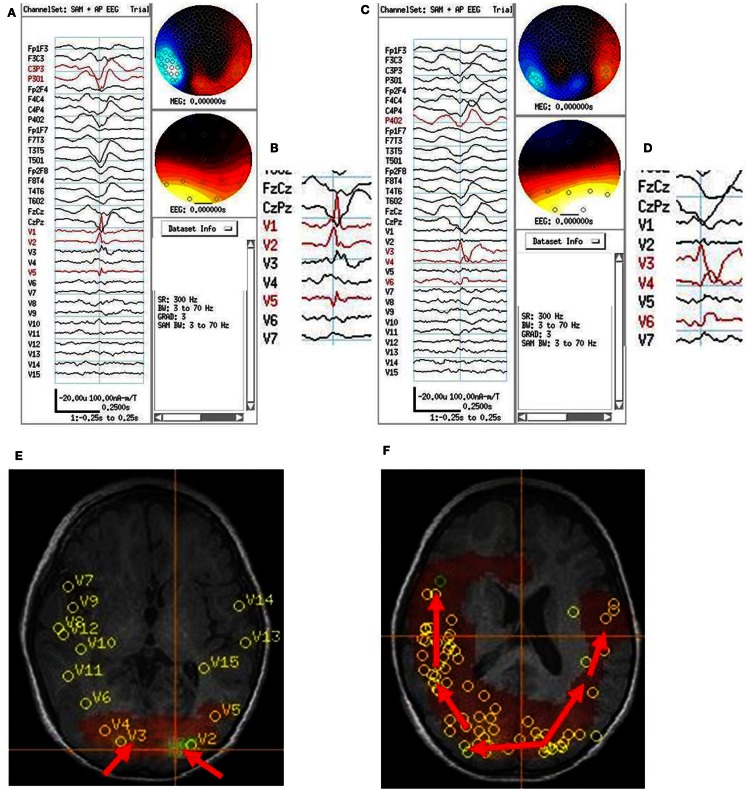
Non-invasive studies to predict regions of seizure onset are important for planning intracranial grid locations for invasive cortical recordings prior to resective surgery for patients with medically intractable epilepsy. The neurosurgeon needs to know both the seizure onset zone (SOZ) and the region of immediate cortical spread to determine the epileptogenic zone to be resected. The immediate zone of spread may be immediately adjacent, on a nearby gyrus, in a different lobe, and sometimes even in the contralateral cerebral hemisphere. We reviewed consecutive simultaneous EEG/MEG recordings on 162 children with medically intractable epilepsy. We analyzed the MEG signals in the bandwidth 20-70 Hz with a beamformer algorithm, synthetic aperture magnetometry, at a 2.5 mm voxel spacing throughout the brain (virtual sensor locations, VSLs) with the kurtosis statistic (g 2) to determine presence of excess kurtosis (γ2) consistent with intermittent increased high frequency spikiness of the background. The MEG time series was reconstructed (virtual sensor signals) at each of these VSLs. The VS signals were further examined with a relative peak amplitude spike detection algorithm. The time of VS spike detection was compared to the simultaneous EEG and MEG sensor signals for presence of conventional epileptiform spike morphology in the latter signals. The time of VS spike detection was compared across VSLs to determine earliest and last VSL to show a VS spike. Seven subjects showed delay in activation across VS locations detectable on visual examination. We compared the VS locations that showed earliest and later VS spikes with the locations on intracranial grid locations by electrocorticography (ECoG) that showed spikes and both onset and spread of seizures. We compared completeness of resection of VS locations to postoperative outcome. The VS locations for spike onset and spread were similar to locations for ictal onset and spread by ECoG.
非侵入性研究预测癫痫起始区对于计划在致痫性皮层切除术前进行颅内网格定位具有重要意义,对于药物难治性癫痫患者来说。神经外科医生需要知道癫痫起始区 (SOZ) 和即刻皮质扩散区,以确定要切除的致痫区。即刻扩散区可能紧邻、在附近脑回、在不同脑叶,甚至在对侧大脑半球。我们回顾了 162 例药物难治性癫痫儿童连续同步 EEG/MEG 记录。我们使用波束形成算法分析了 20-70 Hz 带宽内的 MEG 信号,使用合成孔径磁强计在整个大脑中以 2.5 毫米体素间距 (虚拟传感器位置,VSL) 进行分析,使用峰度统计量 (g2) 确定是否存在异常峰度 (γ2),与背景高频尖峰间歇性增加一致。在每个 VSL 处重建 MEG 时间序列 (虚拟传感器信号)。对 VS 信号进一步使用相对峰值幅度尖峰检测算法进行检查。比较 VS 尖峰检测时间与同时进行的 EEG 和 MEG 传感器信号,以检测后者信号中是否存在常规癫痫样尖峰形态。比较 VSL 之间的 VS 尖峰检测时间,以确定最早和最晚出现 VS 尖峰的 VSL。7 例患者表现出在视觉检查可检测到的 VSL 之间的激活延迟。我们将显示最早和最晚 VS 尖峰的 VS 位置与颅内网格位置的 ECoG 上显示尖峰和癫痫发作起始和扩散的位置进行比较。我们比较了 VS 位置的完全切除与术后结果。VS 位置的起始和扩散与 ECoG 上的起始和扩散相似。