Department of Paediatric Infectious Diseases and Immunology, Erasmus MC-Sophia, Rotterdam, The Netherlands.
PLoS Med. 2013;10(5):e1001444. doi: 10.1371/journal.pmed.1001444. Epub 2013 May 14.
Mycoplasma pneumoniae is thought to be a common cause of respiratory tract infections (RTIs) in children. The diagnosis of M. pneumoniae RTIs currently relies on serological methods and/or the detection of bacterial DNA in the upper respiratory tract (URT). It is conceivable, however, that these diagnostic methods also yield positive results if M. pneumoniae is carried asymptomatically in the URT. Positive results from these tests may therefore not always be indicative of a symptomatic infection. The existence of asymptomatic carriage of M. pneumoniae has not been established. We hypothesized that asymptomatic carriage in children exists and investigated whether colonization and symptomatic infection could be differentiated by current diagnostic methods.
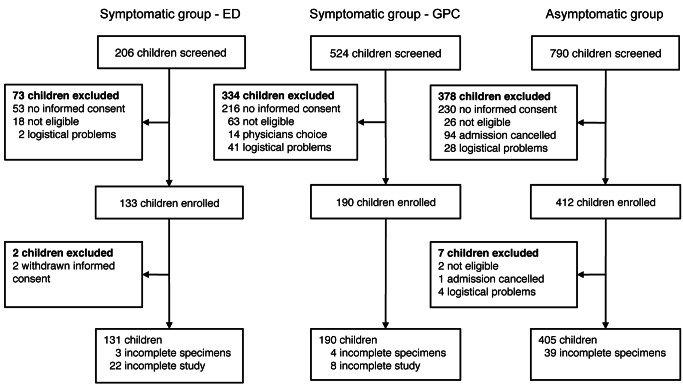
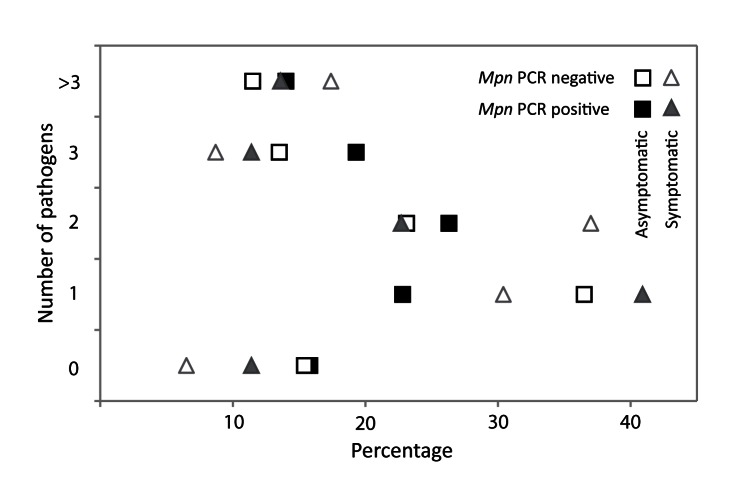
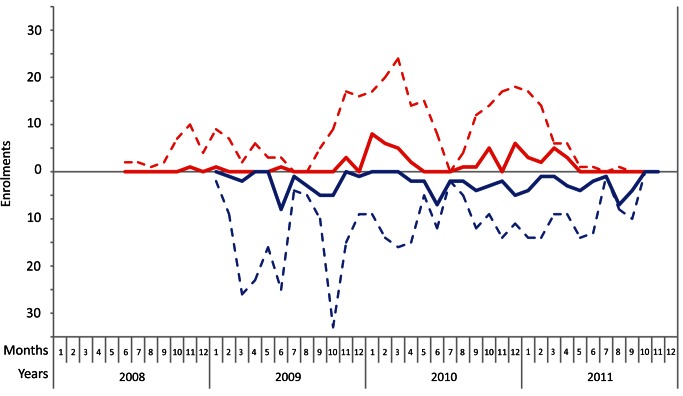
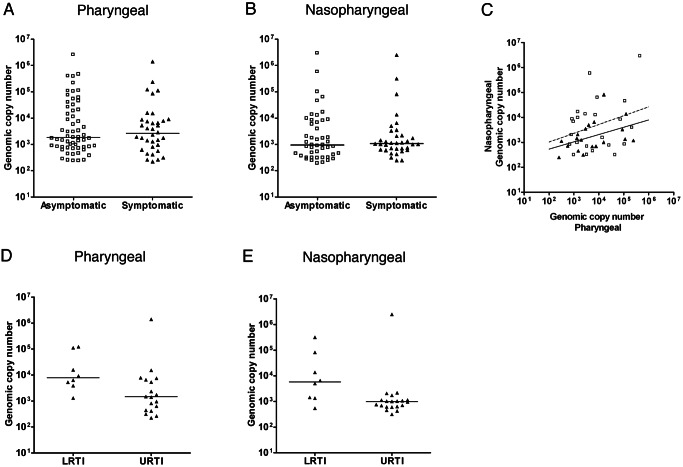
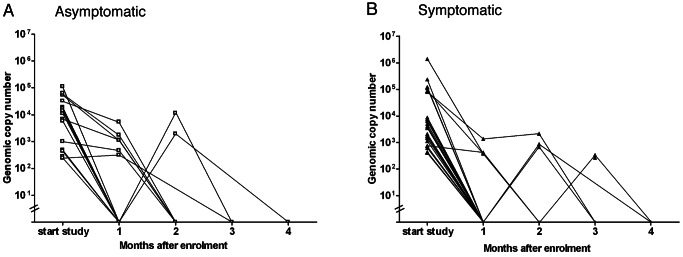
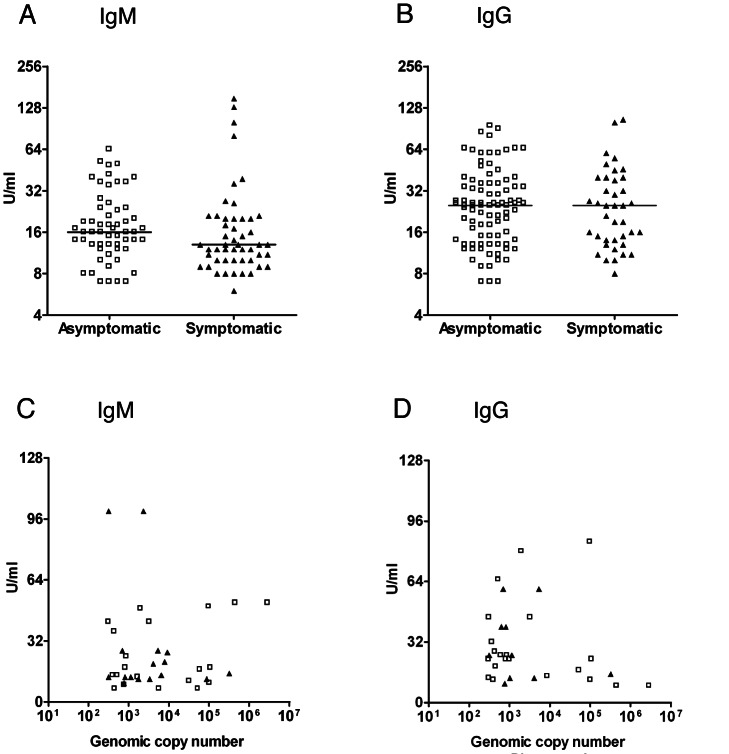
This study was conducted at the Erasmus MC-Sophia Children's Hospital and the after-hours General Practitioners Cooperative in Rotterdam, The Netherlands. Asymptomatic children (n = 405) and children with RTI symptoms (n = 321) aged 3 mo to 16 y were enrolled in a cross-sectional study from July 1, 2008, to November 30, 2011. Clinical data, pharyngeal and nasopharyngeal specimens, and serum samples were collected. The primary objective was to differentiate between colonization and symptomatic infection with M. pneumoniae by current diagnostic methods, especially real-time PCR. M. pneumoniae DNA was detected in 21.2% (95% CI 17.2%-25.2%) of the asymptomatic children and in 16.2% (95% CI 12.2%-20.2%) of the symptomatic children (p = 0.11). Neither serology nor quantitative PCR nor culture differentiated asymptomatic carriage from infection. A total of 202 children were tested for the presence of other bacterial and viral pathogens. Two or more pathogens were found in 56% (63/112) of the asymptomatic children and in 55.5% (50/90) of the symptomatic children. Finally, longitudinal sampling showed persistence of M. pneumoniae in the URT for up to 4 mo. Fifteen of the 21 asymptomatic children with M. pneumoniae and 19 of the 22 symptomatic children with M. pneumoniae in this longitudinal follow-up tested negative after 1 mo.
Although our study has limitations, such as a single study site and limited sample size, our data indicate that the presence of M. pneumoniae in the URT is common in asymptomatic children. The current diagnostic tests for M. pneumoniae are unable to differentiate between asymptomatic carriage and symptomatic infection.
肺炎支原体被认为是儿童呼吸道感染(RTIs)的常见病因。目前,肺炎支原体 RTIs 的诊断依赖于血清学方法和/或上呼吸道(URT)中细菌 DNA 的检测。然而,可以想象,如果肺炎支原体在 URT 中无症状携带,这些诊断方法也会产生阳性结果。因此,这些检测的阳性结果并不总是表明存在有症状的感染。无症状携带肺炎支原体的情况尚未确定。我们假设儿童中存在无症状携带,并研究当前的诊断方法是否可以区分定植和有症状的感染。
这项研究在荷兰鹿特丹伊拉斯谟 MC-索菲亚儿童医院和下班后全科医生合作医院进行。2008 年 7 月 1 日至 2011 年 11 月 30 日,我们招募了年龄在 3 个月至 16 岁之间的无症状儿童(n = 405)和有 RTI 症状的儿童(n = 321)进行横断面研究。收集临床数据、咽和鼻咽标本以及血清样本。主要目的是通过当前的诊断方法,特别是实时 PCR,区分肺炎支原体的定植和有症状的感染。在 21.2%(95%CI 17.2%-25.2%)的无症状儿童和 16.2%(95%CI 12.2%-20.2%)的有症状儿童中检测到肺炎支原体 DNA(p = 0.11)。血清学、定量 PCR 或培养均无法区分无症状携带与感染。共有 202 名儿童接受了其他细菌和病毒病原体的检测。在 56%(63/112)的无症状儿童和 55.5%(50/90)的有症状儿童中发现了两种或两种以上的病原体。最后,纵向采样显示肺炎支原体可在上呼吸道持续存在长达 4 个月。在这项纵向随访中,21 名无症状携带肺炎支原体的儿童中有 15 名和 22 名有症状携带肺炎支原体的儿童中有 19 名在 1 个月后检测结果为阴性。
尽管我们的研究存在局限性,例如单一研究地点和有限的样本量,但我们的数据表明,肺炎支原体在上呼吸道无症状携带的情况在无症状儿童中很常见。目前用于肺炎支原体的诊断检测方法无法区分无症状携带和有症状的感染。