Kids Cancer Centre, Sydney Children's Hospital, Randwick, NSW, Australia.
Pediatr Blood Cancer. 2013 Sep;60(9):1520-7. doi: 10.1002/pbc.24559. Epub 2013 Jun 3.
Over the last 25 years, donor source, conditioning, graft-versus-host disease prevention and supportive care for children undergoing hematopoeitic stem cell transplantation (HSCT) have changed dramatically. HSCT indications for acute lymphoblastic leukemia (ALL) now include high-risk patients in first and subsequent remission. There is a large burden of infectious and pre-HSCT morbidities, due to myelosuppressive therapy required for remission induction. We hypothesized that, despite these trends, overall survival (OS) had increased.
A retrospective audit of allogeneic pediatric HSCT for ALL was performed in our institution over 25 years. Outcomes for 136 HSCTs were analyzed in three consecutive 8-year periods (Period 1: 1/1/1984-31/8/1992, Period 2: 1/9/1992-30/4/2001, Period 3: 1/5/2001-31/12/2009).
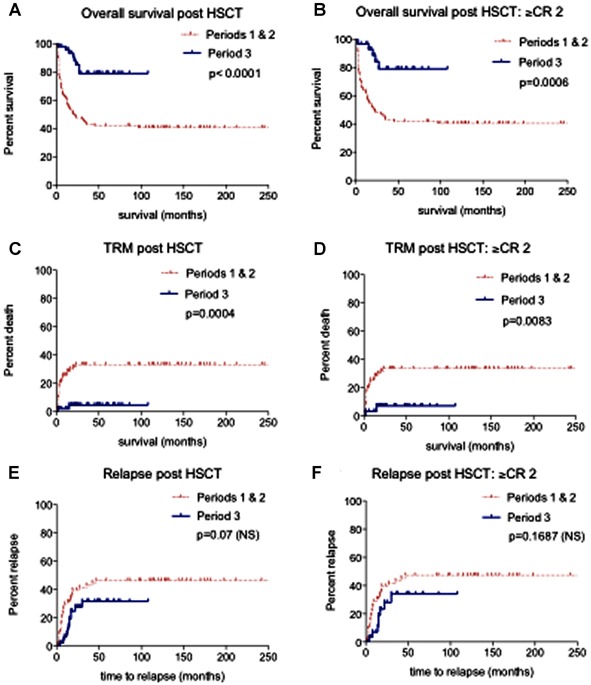
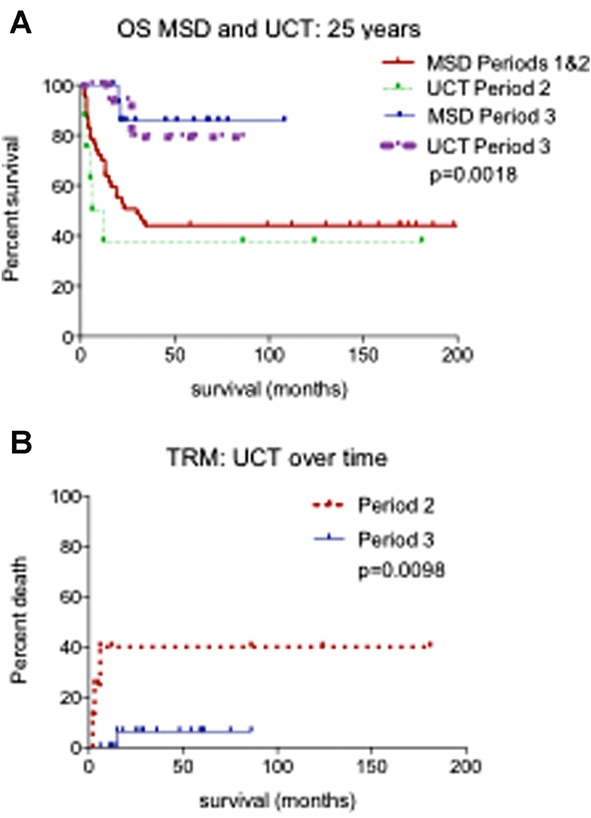
Despite a significant increase in unrelated donor HSCT, event-free and OS over 25 years improved significantly. (EFS 31.6-64.8%, P = 0.0027; OS 41.8-78.9%, P < 0.0001) Concurrently, TRM dropped from 33% to 5% (P = 0.0004) whilst relapse rate was static (P = 0.07). TRM reduced significantly for matched sibling and unrelated cord blood transplantation (UCT) in Period 3 compared with earlier periods (P = 0.036, P = 0.0098, respectively). Factors leading to improved survival in patients undergoing UCT include better matching, higher total nucleated cell doses, and significantly faster neutrophil engraftment. Length of initial HSCT admission was similar over time.
EFS and OS have increased significantly despite heightened HSCT complexity. This survival gain was due to TRM reduction. Contemporary patients have benefited from refined donor selection and improved supportive care. Overall rates of leukemic relapse post-HSCT are unchanged, and remain the focus for improvement.
在过去的 25 年中,供者来源、预处理、移植物抗宿主病预防和造血干细胞移植(HSCT)后的支持治疗发生了巨大变化。HSCT 适应证现已包括首次缓解和后续缓解的高危急性淋巴细胞白血病(ALL)患者。由于缓解诱导需要进行骨髓抑制性治疗,因此存在大量感染和 HSCT 前合并症。我们假设,尽管存在这些趋势,但总体生存率(OS)仍有所提高。
对本机构 25 年来所有接受 ALL 异基因 HSCT 的患儿进行回顾性审核。对三个连续 8 年期间的 136 例 HSCT 结果进行分析(第 1 期:1984 年 1 月 1 日-1992 年 8 月 31 日;第 2 期:1992 年 9 月 1 日-2001 年 4 月 30 日;第 3 期:2001 年 5 月 1 日-2009 年 12 月 31 日)。
尽管无关供者 HSCT 显著增加,但 25 年来无事件生存率和 OS 均显著提高。(EFS 为 31.6%-64.8%,P=0.0027;OS 为 41.8%-78.9%,P<0.0001)同时,TRM 从 33%降至 5%(P=0.0004),而复发率保持不变(P=0.07)。与早期相比,第 3 期匹配同胞和无关脐带血移植(UCT)的 TRM 显著降低(P=0.036,P=0.0098)。导致 UCT 患者生存改善的因素包括更好的匹配、更高的总核细胞剂量以及更快的中性粒细胞植入。初始 HSCT 住院时间随时间推移而相似。
尽管 HSCT 变得更加复杂,但 EFS 和 OS 仍显著提高。这种生存获益归因于 TRM 降低。当代患者受益于供者选择的精细化和支持治疗的改善。HSCT 后白血病复发的总体发生率保持不变,仍是改善的重点。