Gregson S, Nyamukapa C, Schumacher C, Magutshwa-Zitha S, Skovdal M, Yekeye R, Sherr L, Campbell C
Department of Infectious Disease Epidemiology, Imperial College London, London, UK.
AIDS Care. 2013;25 Suppl 1(Suppl 1):S88-96. doi: 10.1080/09540121.2012.748171.
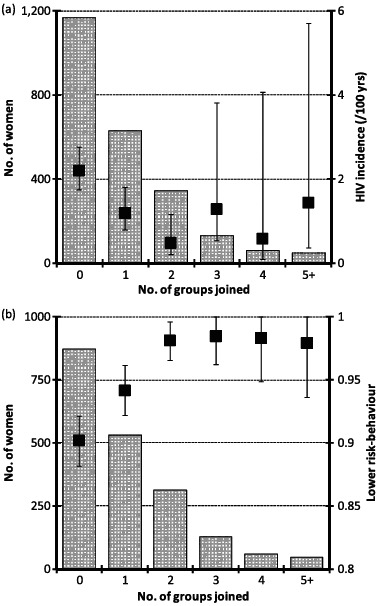
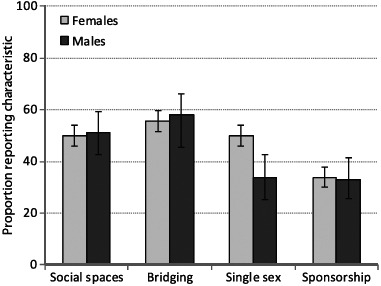
Membership of indigenous local community groups was protective against HIV for women, but not for men, in eastern Zimbabwe during the period of greatest risk reduction (1999-2004). We use four rounds of data from a population cohort to investigate: (1) the effects of membership of multiple community groups during this period; (2) the effects of group membership in the following five years; and (3) the effects of characteristics of groups hypothesised to determine their effect on HIV risk. HIV incidence from 1998 to 2003 was 1.18% (95% CI: 0.78-1.79%), 0.48% (0.20-1.16%) and 1.13% (0.57-2.27%), in women participating in one, two and three or more community groups at baseline versus 2.19% (1.75-2.75%) in other women. In 2003-2005, 36.5% (versus 43% in 1998-2000) of women were members of community groups, 50% and 56% of which discussed HIV prevention and met with other groups, respectively; the corresponding figures for men were 24% (versus 28% in 1998-2000), 51% and 58%. From 2003 to 2008, prior membership of community groups was no longer protective against HIV for women (1.13% versus 1.29%, aIRR = 1.25; p = 0.23). However, membership of groups that provided social spaces for dialogue about HIV prevention (0.62% versus 1.01%, aIRR = 0.54; p = 0.28) and groups that interacted with other groups (0.65% versus 1.01%, aIRR = 0.51; p = 0.19) showed non-significant protective effects. For women, membership of a group with external sponsorship showed a non-significant increase in HIV risk compared to membership of unsponsored groups (adjusted odds ratio = 1.63, p = 0.48). Between 2003 and 2008, membership of community groups showed a non-significant tendency towards higher HIV risk for men (1.47% versus 0.94%, p = 0.23). Community responses contributed to HIV decline in eastern Zimbabwe. Sensitive engagement and support for local groups (including non-AIDS groups) to encourage dialogue on positive local responses to HIV and to challenge harmful social norms and incorrect information could enhance HIV prevention.
在津巴布韦东部风险降低最显著的时期(1999 - 2004年),当地土著社区团体成员身份对女性预防艾滋病毒具有保护作用,但对男性则不然。我们使用来自一个人群队列的四轮数据进行调查:(1)在此期间加入多个社区团体的影响;(2)接下来五年团体成员身份的影响;(3)假设能决定其对艾滋病毒风险影响的团体特征的影响。1998年至2003年,基线时参加一个、两个及三个或更多社区团体的女性艾滋病毒发病率分别为1.18%(95%置信区间:0.78 - 1.79%)、0.48%(0.20 - 1.16%)和1.13%(0.57 - 2.27%),而其他女性为2.19%(1.75 - 2.75%)。在2003 - 2005年,36.5%的女性是社区团体成员(1998 - 2000年为43%),其中分别有50%和56%的团体讨论艾滋病毒预防并与其他团体会面;男性的相应数字分别为24%(1998 - 2000年为28%)、51%和58%。从2003年到2008年,社区团体先前的成员身份对女性预防艾滋病毒不再具有保护作用(1.13%对1.29%,调整后的发病率比 = 1.25;p = 0.23)。然而,为艾滋病毒预防提供对话社会空间的团体成员(0.62%对1.01%,调整后的发病率比 = 0.54;p = 0.28)以及与其他团体互动的团体成员(0.65%对1.01%,调整后的发病率比 = 0.51;p = 0.19)显示出不显著的保护作用。对于女性,与无外部资助团体的成员相比,有外部资助团体的成员感染艾滋病毒的风险有不显著增加(调整后的优势比 = 1.63,p = 0.48)。在2003年至2008年期间,社区团体成员身份对男性显示出艾滋病毒风险有不显著的升高趋势(1.47%对0.94%,p = 0.23)。社区应对措施促使津巴布韦东部艾滋病毒感染率下降。对当地团体(包括非艾滋病团体)进行敏感的参与和支持,以鼓励就当地对艾滋病毒的积极应对措施展开对话,并挑战有害的社会规范和错误信息,可能会加强艾滋病毒预防工作。