Pulmonary and Critical Care Medicine Division, Washington Hospital Center, Washington, District of Columbia, USA.
BMJ Open. 2013 Jun 20;3(6):e002898. doi: 10.1136/bmjopen-2013-002898.
Streptococcus pneumoniae (SP) represents a major pathogen in pneumonia. The impact of azithromycin on mortality in SP pneumonia remains unclear. Recent safety concerns regarding azithromycin have raised alarm about this agent's role with pneumonia. We sought to clarify the relationship between survival and azithromycin use in SP pneumonia.
Retrospective cohort.
Urban academic hospital.
Adults with a diagnosis of SP pneumonia (January-December 2010). The diagnosis of pneumonia required a compatible clinical syndrome and radiographic evidence of an infiltrate.
None.
Hospital mortality served as the primary endpoint, and we compared patients given azithromycin with those not treated with this. Covariates of interest included demographics, severity of illness, comorbidities and infection-related characteristics (eg, appropriateness of initial treatment, bacteraemia). We employed logistic regression to assess the independent impact of azithromycin on hospital mortality.
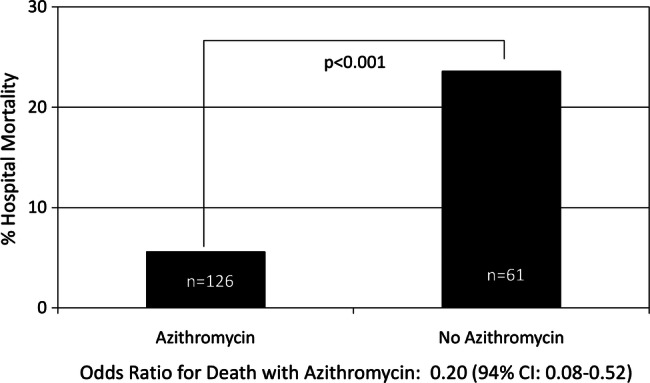
The cohort included 187 patients (mean age: 67.0±8.2 years, 50.3% men, 5.9% admitted to the intensive care unit). The most frequently utilised non-macrolide antibiotics included: ceftriaxone (n=111), cefepime (n=31) and moxifloxacin (n=22). Approximately two-thirds of the cohort received azithromycin. Crude mortality was lower in persons given azithromycin (5.6% vs 23.6%, p<0.01). The final survival model included four variables: age, need for mechanical ventilation, initial appropriate therapy and azithromycin use. The adjusted OR for mortality associated with azithromycin equalled 0.26 (95% CI 0.08 to 0.80, p=0.018).
SP pneumonia generally remains associated with substantial mortality while azithromycin treatment is associated with significantly higher survival rates. The impact of azithromycin is independent of multiple potential confounders.
肺炎链球菌(SP)是肺炎的主要病原体。阿奇霉素对 SP 肺炎死亡率的影响尚不清楚。最近有关阿奇霉素的安全性问题引起了人们对该药物在肺炎治疗中作用的担忧。我们旨在明确 SP 肺炎患者生存与阿奇霉素使用之间的关系。
回顾性队列研究。
城市学术医院。
2010 年 1 月至 12 月期间被诊断为 SP 肺炎的成年人。肺炎的诊断需要符合临床综合征,并伴有浸润性放射影像学证据。
无。
住院死亡率为主要终点,我们比较了接受阿奇霉素治疗和未接受该治疗的患者。感兴趣的协变量包括人口统计学、疾病严重程度、合并症和感染相关特征(例如初始治疗的适当性、菌血症)。我们采用逻辑回归评估阿奇霉素对住院死亡率的独立影响。
该队列包括 187 名患者(平均年龄:67.0±8.2 岁,50.3%为男性,5.9%收入重症监护病房)。最常使用的非大环内酯类抗生素包括:头孢曲松(n=111)、头孢吡肟(n=31)和莫西沙星(n=22)。约三分之二的患者接受了阿奇霉素治疗。接受阿奇霉素治疗的患者死亡率较低(5.6%比 23.6%,p<0.01)。最终的生存模型包括四个变量:年龄、需要机械通气、初始适当治疗和阿奇霉素使用。与阿奇霉素相关的死亡率调整后的 OR 为 0.26(95%CI 0.08 至 0.80,p=0.018)。
SP 肺炎的死亡率仍然很高,而阿奇霉素治疗与显著更高的生存率相关。阿奇霉素的影响独立于多个潜在混杂因素。