Warwick Orthopaedics, Warwick Medical School, University of Warwick, Coventry, UK.
BMJ Open. 2013 Jun 25;3(6):e002583. doi: 10.1136/bmjopen-2013-002583.
To quantify and draw inferences on the clinical effectiveness of platelet-rich therapy in the management of patients with a typical osteoporotic fracture of the hip.
Single centre, parallel group, participant-blinded, randomised controlled trial.
UK Major Trauma Centre.
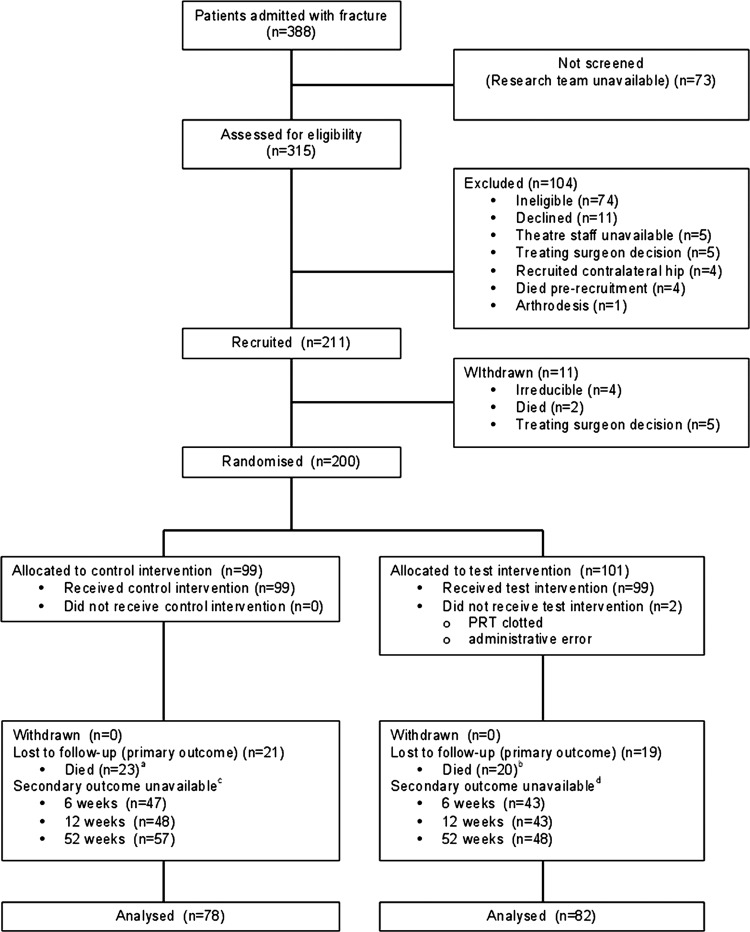
200 of 315 eligible patients aged 65 years and over with any type of intracapsular fracture of the proximal femur. Patients were excluded if their fracture precluded internal fixation.
Participants underwent internal fixation of the fracture with cannulated screws and were randomly allocated to receive an injection of platelet-rich plasma into the fracture site or not.
Failure of fixation within 12 months, defined as any revision surgery.
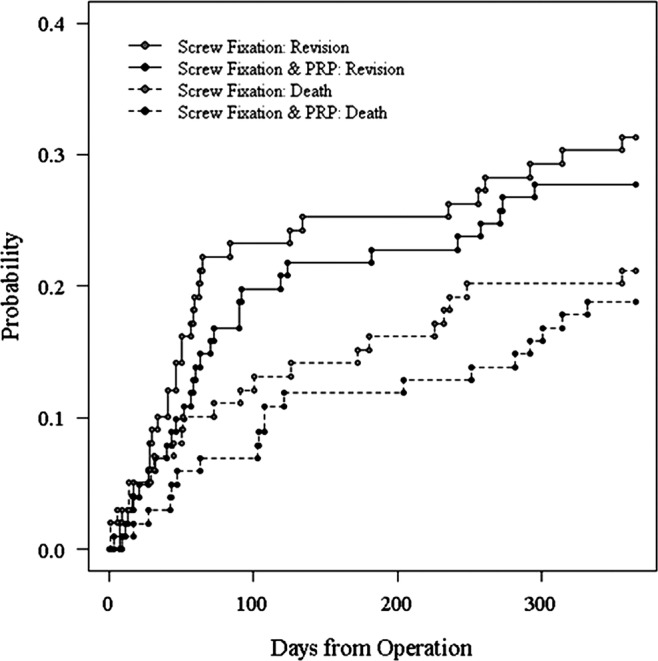
Primary outcome data were available for 82 of 101 and 78 of 99 participants allocated to test and control groups, respectively; the remainder died prior to final follow-up. There was an absolute risk reduction of 5.6% (95% CI -10.6% to 21.8%) favouring treatment with platelet-rich therapy (χ(2) test, p=0.569). An adjusted effect estimate from a logistic regression model was similar (OR=0.71, 95% CI 0.36 to 1.40, z test; p=0.325). There were no significant differences in any of the secondary outcome measures excepting length of stay favouring treatment with platelet-rich therapy (median difference 8 days, Mann-Whitney U test; p=0.03). The number and distribution of adverse events were similar. Estimated cumulative incidence functions for the competing events of death and revision demonstrated no evidence of a significant treatment effect (HR 0.895, 95% CI 0.533 to 1.504; p=0.680 in favour of platelet-rich therapy).
No evidence of a difference in the risk of revision surgery within 1 year in participants treated with platelet-rich therapy compared with those not treated. However, we cannot definitively exclude a clinically meaningful difference.
Current Controlled Trials, ISRCTN49197425, http://www.controlled-trials.com/ISRCTN49197425.
定量评估并推断富含血小板的治疗在管理典型髋部骨质疏松性骨折患者中的临床效果。
单中心、平行组、参与者设盲、随机对照试验。
英国大型创伤中心。
200 名符合条件的 65 岁及以上患者,患有任何类型的囊内股骨近端骨折。如果患者的骨折妨碍了内固定,则将其排除在外。
参与者接受空心螺钉内固定骨折,并随机分配接受或不接受富含血小板的血浆注射到骨折部位。
12 个月内固定失败,定义为任何翻修手术。
101 名参与者中,有 82 名和 99 名参与者分别分配到试验组和对照组,有主要结局数据;其余参与者在最终随访前死亡。富含血小板治疗组的绝对风险降低了 5.6%(95%CI-10.6%至 21.8%)(卡方检验,p=0.569)。逻辑回归模型的调整后效应估计值也相似(OR=0.71,95%CI 0.36 至 1.40,z 检验;p=0.325)。除了富含血小板治疗组的住院时间更有利外,其他次要结局指标均无显著差异(中位数差异 8 天,Mann-Whitney U 检验;p=0.03)。不良事件的数量和分布相似。对死亡和翻修这两种竞争事件的估计累积发生率函数没有表明治疗效果有显著差异(HR 0.895,95%CI 0.533 至 1.504;p=0.680 有利于富含血小板治疗)。
与未接受富含血小板治疗的患者相比,接受富含血小板治疗的患者在 1 年内接受翻修手术的风险没有差异。然而,我们不能明确排除具有临床意义的差异。
当前对照试验,ISRCTN49197425,http://www.controlled-trials.com/ISRCTN49197425。