Fisher Sheila A, Dorée Carolyn, Brunskill Susan J, Mathur Anthony, Martin-Rendon Enca
Systematic Review Initiative, NHS Blood and Transplant, John Radcliffe Hospital, Oxford, United Kingdom ; Nuffield Division of Clinical Laboratory Sciences, Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom.
PLoS One. 2013 Jun 19;8(6):e64669. doi: 10.1371/journal.pone.0064669. Print 2013.
To evaluate bone marrow stem cell treatment (BMSC) in patients with ischemic heart disease (IHD) and no option of revascularization.
Autologous BMSC therapy has emerged as a novel approach to treat patients with acute myocardial infarction or chronic ischemia and heart failure following percutaneous or surgical revascularization, respectively. However, the effect of the treatment has not been systematic evaluated in patients who are not eligible for revascularization.
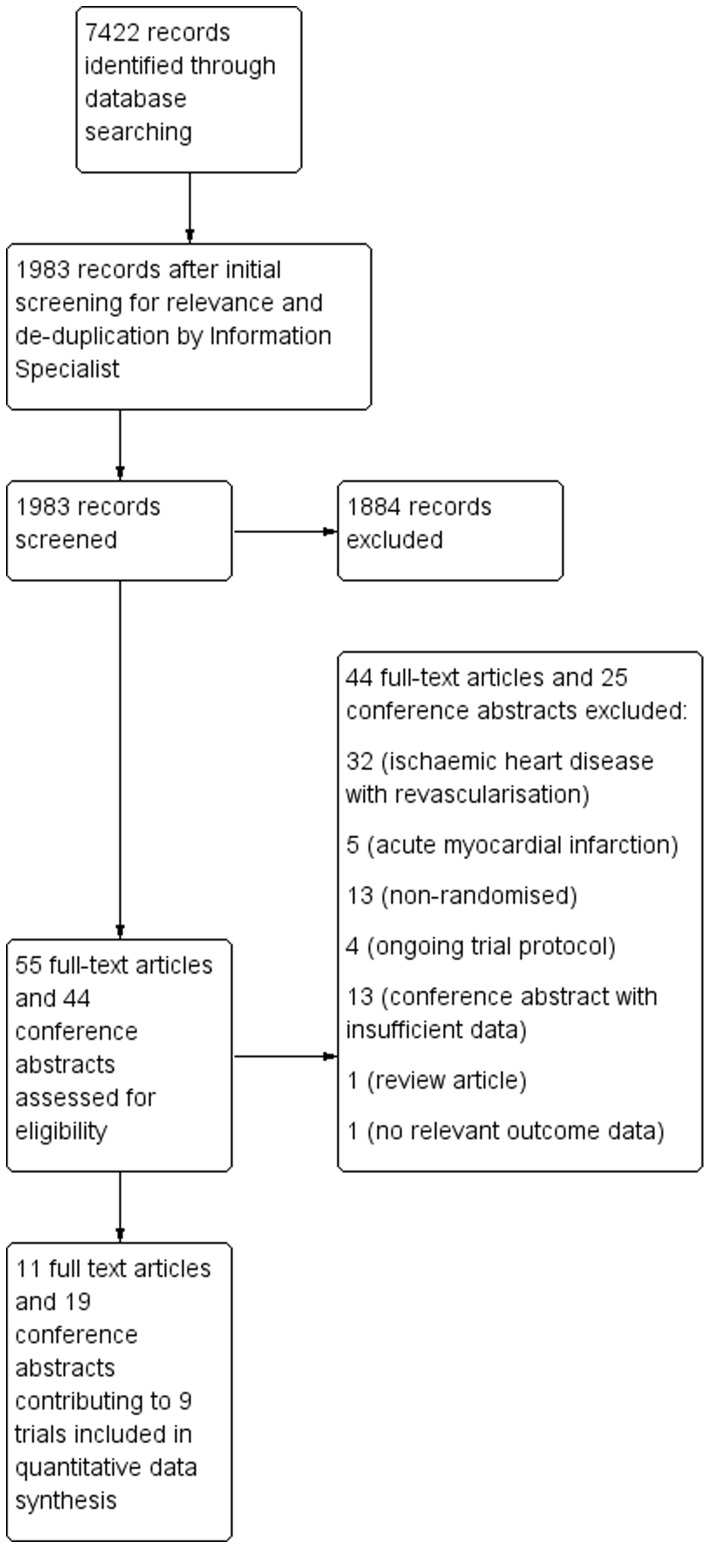
MEDLINE (1950-2012), EMBASE (1980-2012), CENTRAL (The Cochrane Library 2012, Issue 8) and ongoing trial databases were searched for relevant randomized controlled trials. Trials where participants were diagnosed with IHD, with no option for revascularization and who received any dose of stem cells by any delivery route were selected for inclusion. Study and participant characteristics, details of the intervention and comparator, and outcomes measured were recorded by two reviewers independently. Primary outcome measures were defined as mortality and measures of angina; secondary outcomes were heart failure, quality of life measures, exercise/performance and left ventricular ejection fraction (LVEF).
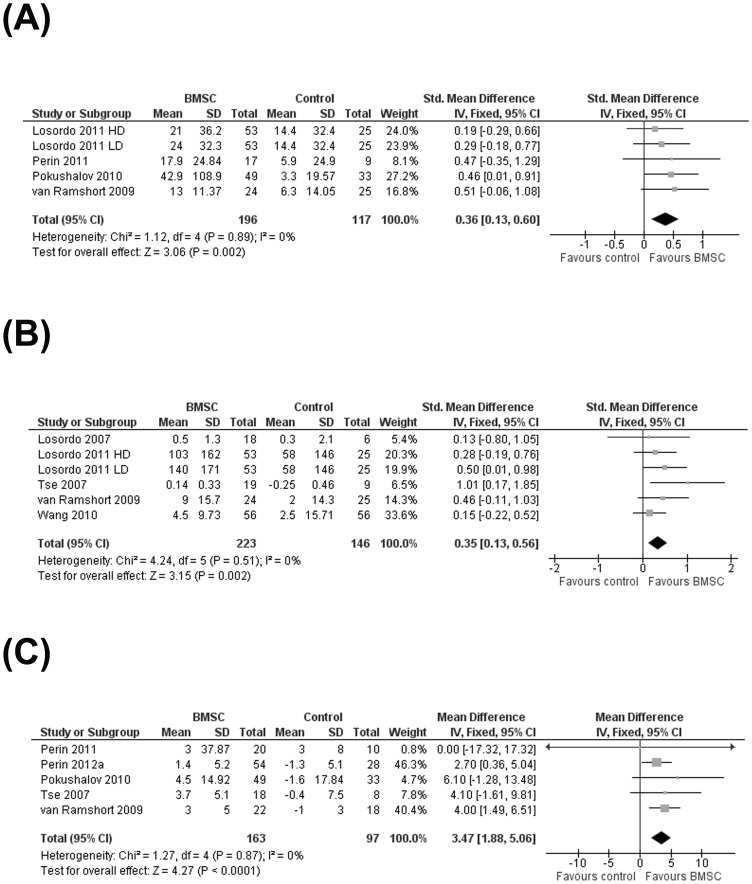
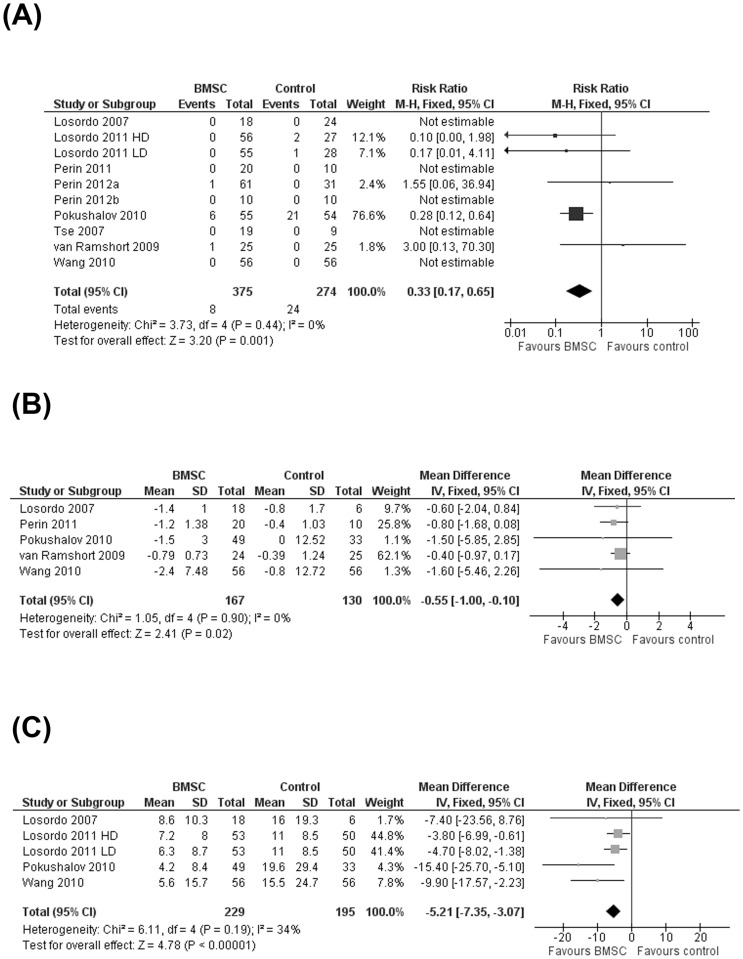
Nine trials were eligible for inclusion. BMSC treatment significantly reduced the risk of mortality (Relative Risk 0.33; 95% Confidence Interval 0.17 to 0.65; P = 0.001). Patients who received BMSC showed a significantly greater improvement in CCS angina class (Mean Difference -0.55; 95% Confidence Interval -1.00 to -0.10; P = 0.02) and significantly fewer angina episodes per week at the end of the trial (Mean Difference -5.21; 95% Confidence Interval -7.35 to -3.07; P<0.00001) than those who received no BMSC. In addition, the treatment significantly improved quality of life, exercise/performance and LVEF in these patients.
BMSC treatment has significant clinical benefit as stand-alone treatment in patients with IHD and no other treatment option. These results require confirmation in large well-powered trials with long-term follow-up to fully evaluate the clinical efficacy of this treatment.
评估骨髓干细胞治疗(BMSC)对无法进行血运重建的缺血性心脏病(IHD)患者的疗效。
自体BMSC治疗已成为一种新的治疗方法,分别用于治疗经皮或外科血运重建术后的急性心肌梗死患者或慢性缺血及心力衰竭患者。然而,对于不适合进行血运重建的患者,该治疗效果尚未得到系统评估。
检索MEDLINE(1950 - 2012年)、EMBASE(1980 - 2012年)、CENTRAL(考克兰图书馆2012年第8期)及正在进行的试验数据库,查找相关随机对照试验。纳入标准为:参与者被诊断为IHD,无法进行血运重建,且通过任何给药途径接受任何剂量干细胞治疗的试验。两名研究者独立记录研究和参与者特征、干预措施及对照的详细信息以及所测量的结局。主要结局指标定义为死亡率和心绞痛指标;次要结局包括心力衰竭、生活质量指标、运动/功能及左心室射血分数(LVEF)。
9项试验符合纳入标准。BMSC治疗显著降低了死亡风险(相对风险0.33;95%置信区间0.17至0.65;P = 0.001)。接受BMSC治疗的患者在加拿大心血管学会(CCS)心绞痛分级方面改善更为显著(平均差值 -0.55;95%置信区间 -1.00至 -0.10;P = 0.02),且在试验结束时每周心绞痛发作次数显著少于未接受BMSC治疗的患者(平均差值 -5.21;95%置信区间 -7.35至 -3.07;P < 0.00001)。此外,该治疗显著改善了这些患者的生活质量、运动/功能及LVEF。
对于无其他治疗选择的IHD患者,BMSC治疗作为单一治疗具有显著临床益处。这些结果需要在大规模、有充分效力且长期随访的试验中得到证实,以全面评估该治疗的临床疗效。