Messier Stephen P, Mihalko Shannon L, Beavers Daniel P, Nicklas Barbara J, DeVita Paul, Carr J Jeffery, Hunter David J, Williamson Jeff D, Bennell Kim L, Guermazi Ali, Lyles Mary, Loeser Richard F
BMC Musculoskelet Disord. 2013 Jul 15;14:208. doi: 10.1186/1471-2474-14-208.
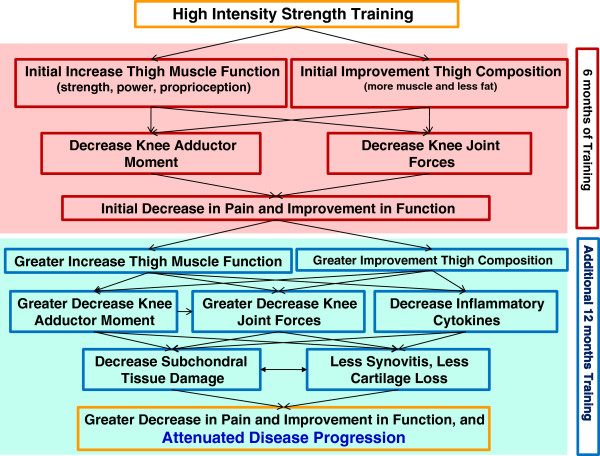
Muscle loss and fat gain contribute to the disability, pain, and morbidity associated with knee osteoarthritis (OA), and thigh muscle weakness is an independent and modifiable risk factor for it. However, while all published treatment guidelines recommend muscle strengthening exercise to combat loss of muscle mass and strength in knee OA patients, previous strength training studies either used intensities or loads below recommended levels for healthy adults or were generally short, lasting only 6 to 24 weeks. The efficacy of high-intensity strength training in improving OA symptoms, slowing progression, and affecting the underlying mechanisms has not been examined due to the unsubstantiated belief that it might exacerbate symptoms. We hypothesize that in addition to short-term clinical benefits, combining greater duration with high-intensity strength training will alter thigh composition sufficiently to attain long-term reductions in knee-joint forces, lower pain levels, decrease inflammatory cytokines, and slow OA progression.
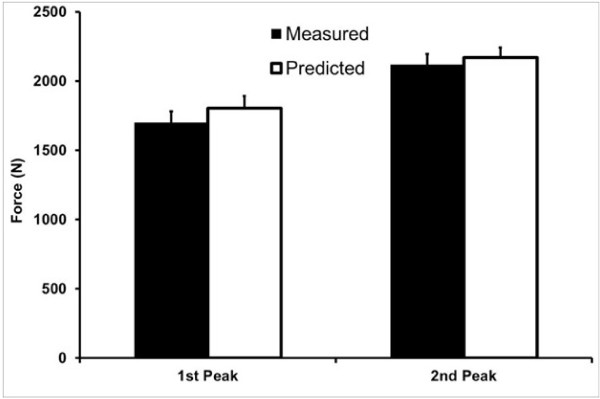
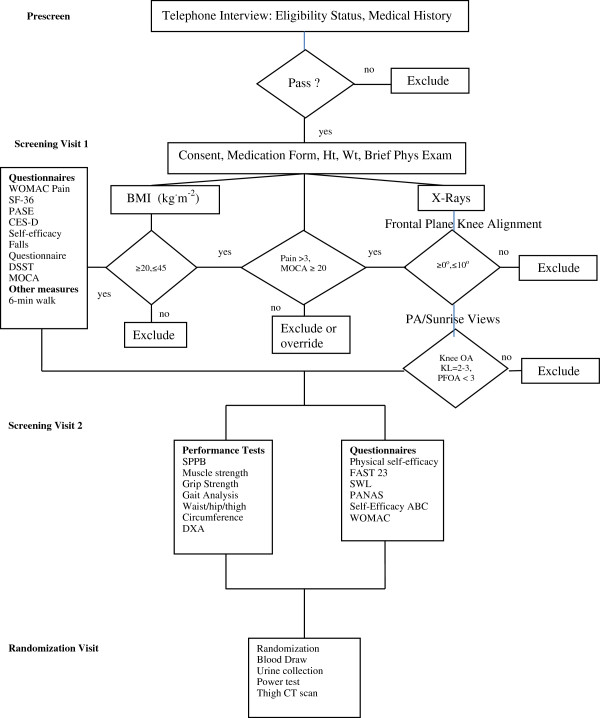
METHODS/DESIGN: This is an assessor-blind, randomized controlled trial. The study population consists of 372 older (age ≥ 55 yrs) ambulatory, community-dwelling persons with: (1) mild-to-moderate medial tibiofemoral OA (Kellgren-Lawrence (KL) = 2 or 3); (2) knee neutral or varus aligned knee ( -2° valgus ≤ angle ≤ 10° varus); (3) 20 kg.m-2 ≥ BMI ≤ 45 kg.m-2; and (3) no participation in a formal strength-training program for more than 30 minutes per week within the past 6 months. Participants are randomized to one of 3 groups: high-intensity strength training (75-90% 1Repetition Maximum (1RM)); low-intensity strength training (30-40%1RM); or healthy living education. The primary clinical aim is to compare the interventions' effects on knee pain, and the primary mechanistic aim is to compare their effects on knee-joint compressive forces during walking, a mechanism that affects the OA disease pathway. Secondary aims will compare the interventions' effects on additional clinical measures of disease severity (e.g., function, mobility); disease progression measured by x-ray; thigh muscle and fat volume, measured by computed tomography (CT); components of thigh muscle function, including hip abductor strength and quadriceps strength, and power; additional measures of knee-joint loading; inflammatory and OA biomarkers; and health-related quality of life.
Test-retest reliability for the thigh CT scan was: total thigh volume, intra-class correlation coefficients (ICC) = 0.99; total fat volume, ICC = 0.99, and total muscle volume, ICC = 0.99. ICC for both isokinetic concentric knee flexion and extension strength was 0.93, and for hip-abductor concentric strength was 0.99. The reliability of our 1RM testing was: leg press, ICC = 0.95; leg curl, ICC = 0.99; and leg extension, ICC = 0.98. Results of this trial will provide critically needed guidance for clinicians in a variety of health professions who prescribe and oversee treatment and prevention of OA-related complications. Given the prevalence and impact of OA and the widespread availability of this intervention, assessing the efficacy of optimal strength training has the potential for immediate and vital clinical impact.
ClinicalTrials.gov, NCT01489462.
肌肉流失和脂肪增加会导致与膝关节骨关节炎(OA)相关的残疾、疼痛和发病率,而大腿肌肉无力是其独立且可改变的风险因素。然而,尽管所有已发表的治疗指南都建议进行肌肉强化锻炼以对抗膝关节OA患者的肌肉量和力量流失,但先前的力量训练研究要么使用低于健康成年人推荐水平的强度或负荷,要么通常持续时间较短,仅为6至24周。由于存在高强度力量训练可能会加重症状的未经证实的观点,其在改善OA症状、减缓疾病进展以及影响潜在机制方面的疗效尚未得到研究。我们假设,除了短期临床益处外,将更长的持续时间与高强度力量训练相结合,将充分改变大腿成分,从而长期降低膝关节受力、减轻疼痛程度、减少炎性细胞因子并减缓OA进展。
方法/设计:这是一项评估者盲法随机对照试验。研究人群包括372名年龄≥55岁的社区居住的能行走的老年人,他们具有以下特征:(1)轻度至中度胫股内侧OA(Kellgren-Lawrence(KL)分级为2或3级);(2)膝关节中立位或内翻(外翻角度≤ -2°且内翻角度≤10°);(3)体重指数(BMI)在20 kg·m⁻²至45 kg·m⁻²之间;(4)在过去6个月内未参加每周超过30分钟的正式力量训练计划。参与者被随机分为3组之一:高强度力量训练(75 - 90%的1次重复最大值(1RM));低强度力量训练(30 - 40%的1RM);或健康生活教育。主要临床目标是比较各干预措施对膝关节疼痛的影响,主要机制目标是比较它们对行走时膝关节压缩力的影响,这是一种影响OA疾病路径的机制。次要目标将比较各干预措施对疾病严重程度的其他临床指标(如功能、活动能力)、通过X线测量的疾病进展、通过计算机断层扫描(CT)测量的大腿肌肉和脂肪体积、大腿肌肉功能的组成部分(包括髋外展肌力量、股四头肌力量和功率)、膝关节负荷的其他测量指标、炎性和OA生物标志物以及健康相关生活质量的影响。
大腿CT扫描的重测信度为:大腿总体积,组内相关系数(ICC)= 0.99;总脂肪体积,ICC = 0.99,总肌肉体积,ICC = 0.99。等速向心膝关节屈伸力量的ICC为0.93,髋外展肌向心力量的ICC为0.99。我们1RM测试的信度为:腿举,ICC = 0.95;腿弯举,ICC = 0.99;腿伸展,ICC = 0.98。该试验结果将为各种健康专业的临床医生提供急需的指导意见,这些医生负责开具和监督OA相关并发症的治疗与预防。鉴于OA的患病率和影响以及这种干预措施的广泛应用,评估最佳力量训练的疗效可能会立即产生至关重要的临床影响。
ClinicalTrials.gov,NCT01489462。