Department of Public Health and Primary Care, University of Cambridge, Cambridge, United Kingdom.
PLoS Med. 2013;10(7):e1001481. doi: 10.1371/journal.pmed.1001481. Epub 2013 Jul 9.
Numerous studies have demonstrated that therapeutic termination of pregnancy (abortion) is associated with an increased risk of subsequent preterm birth. However, the literature is inconsistent, and methods of abortion have changed dramatically over the last 30 years. We hypothesized that the association between previous abortion and the risk of preterm first birth changed in Scotland between 1 January 1980 and 31 December 2008.
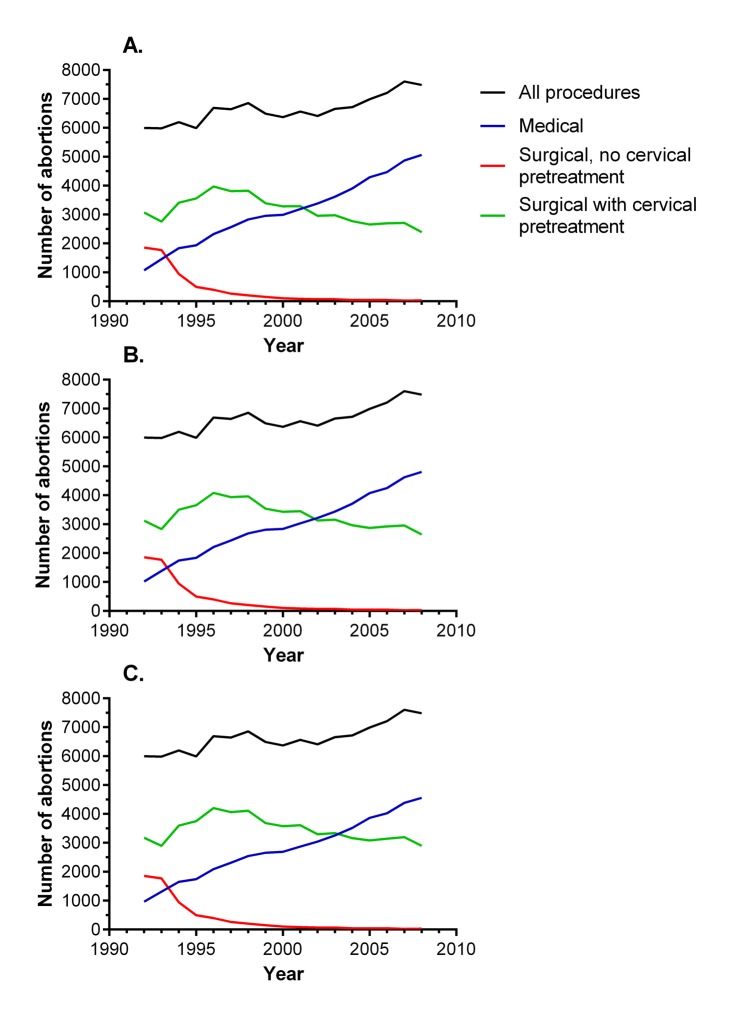
We studied linked Scottish national databases of births and perinatal deaths. We analysed the risk of preterm birth in relation to the number of previous abortions in 732,719 first births (≥24 wk), adjusting for maternal characteristics. The risk (adjusted odds ratio [95% CI]) of preterm birth was modelled using logistic regression, and associations were expressed for a one-unit increase in the number of previous abortions. Previous abortion was associated with an increased risk of preterm birth (1.12 [1.09-1.16]). When analysed by year of delivery, the association was strongest in 1980-1983 (1.32 [1.21-1.43]), progressively declined between 1984 and 1999, and was no longer apparent in 2000-2003 (0.98 [0.91-1.05]) or 2004-2008 (1.02 [0.95-1.09]). A statistical test for interaction between previous abortion and year was highly statistically significant (p<0.001). Analysis of data for abortions among nulliparous women in Scotland 1992-2008 demonstrated that the proportion that were surgical without use of cervical pre-treatment decreased from 31% to 0.4%, and that the proportion of medical abortions increased from 18% to 68%.
Previous abortion was a risk factor for spontaneous preterm birth in Scotland in the 1980s and 1990s, but the association progressively weakened and disappeared altogether by 2000. These changes were paralleled by increasing use of medical abortion and cervical pre-treatment prior to surgical abortion. Although it is plausible that the two trends were related, we could not test this directly as the data on the method of prior abortions were not linked to individuals in the cohort. However, we speculate that modernising abortion methods may be an effective long-term strategy to reduce global rates of preterm birth.
大量研究表明,治疗性终止妊娠(流产)与随后早产的风险增加相关。然而,文献结果并不一致,而且在过去的 30 年中,流产方法发生了巨大变化。我们假设,1980 年 1 月 1 日至 2008 年 12 月 31 日期间,苏格兰以前的流产与早产风险之间的关联发生了变化。
我们研究了苏格兰国家出生和围产儿死亡的相关数据库。我们分析了 732719 例首次分娩(≥24 周)与以前流产次数的关系,调整了产妇特征。使用逻辑回归模型分析早产风险,结果以每增加一次以前流产的单位表示。以前的流产与早产风险增加相关(1.12 [1.09-1.16])。按分娩年份分析时,1980-1983 年的关联最强(1.32 [1.21-1.43]),1984 年至 1999 年逐渐下降,2000-2003 年(0.98 [0.91-1.05])或 2004-2008 年(1.02 [0.95-1.09])不再明显。以前的流产和年份之间的交互作用的统计学检验具有统计学意义(p<0.001)。对苏格兰 1992-2008 年的初产妇流产数据进行分析表明,未行宫颈预处理的手术流产比例从 31%降至 0.4%,而药物流产比例从 18%增至 68%。
在 20 世纪 80 年代和 90 年代,苏格兰以前的流产是自发性早产的一个风险因素,但随着时间的推移,这种关联逐渐减弱,到 2000 年完全消失。这些变化与宫颈预处理前的手术流产中越来越多地使用药物流产和宫颈预处理平行。虽然这两种趋势可能存在关联,但由于无法将以前流产的方法数据与队列中的个体联系起来,我们无法直接进行测试。然而,我们推测,使流产方法现代化可能是降低全球早产率的有效长期策略。