Bixby Center for Population, Health and Sustainability, School of Public Health, University of California at Berkeley, Berkeley, California, USA.
PLoS One. 2013 Jul 12;8(7):e68794. doi: 10.1371/journal.pone.0068794. Print 2013.
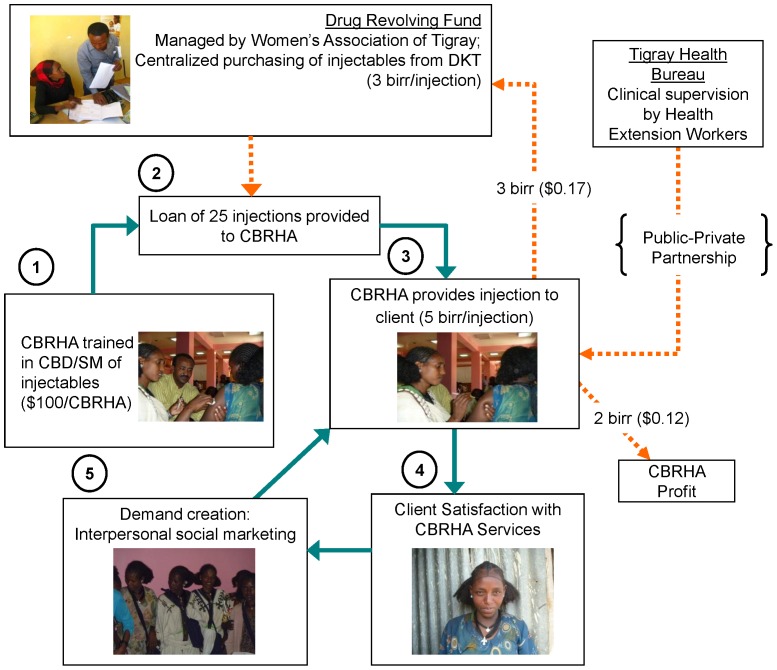
In Sub-Saharan Africa, policy changes have begun to pave the way for community distribution of injectable contraceptives but sustaining such efforts remains challenging. Combining social marketing with community-based distribution provides an opportunity to recover some program costs and compensate workers with proceeds from contraceptive sales. This paper proposes a model for increasing access to injectable contraceptives in rural settings by using community-based distributers as social marketing agents and incorporating financing systems to improve sustainability.
This intervention was implemented in three districts of the Central Zone of Tigray, Ethiopia and program data has been collected from November 2011 through October 2012. A total of 137 Community Based Reproductive Health Agents (CBRHAs) were trained to provide injectable contraceptives and were provided with a loan of 25 injectable contraceptives from a drug revolving fund, created with project funds. The price of a single dose credited to a CBRHA was 3 birr ($0.17) and they provide injections to women for 5 birr ($0.29), determined with willingness-to-pay data. Social marketing was used to create awareness and generate demand. Both quantitative and qualitative methods were used to examine important feasibility aspects of the intervention.
Forty-four percent of CBRHAs were providing family planning methods at the time of the training and 96% believed providing injectable contraceptives would improve their services. By October 2012, 137 CBRHAs had successfully completed training and provided 2541 injections. Of total injections, 47% were provided to new users of injectable contraceptives. Approximately 31% of injections were given for free to the poorest women, including adolescents.
Insights gained from the first year of implementation of the model provide a framework for further expansion in Tigray, Ethiopia. Our experience highlights how program planners can tailor interventions to match family planning preferences and create more sustainable contraceptive service provision with greater impact.
在撒哈拉以南非洲地区,政策的改变已开始为社区分发注射类避孕药具铺平道路,但维持这些努力仍然具有挑战性。将社会营销与基于社区的分发相结合,为从避孕药具销售中收回部分项目成本和补偿工作人员提供了机会。本文提出了一个模型,通过利用基于社区的分销商作为社会营销代理,并纳入融资系统,以提高可持续性,来增加农村地区注射类避孕药具的可及性。
这项干预措施在埃塞俄比亚提格雷中央区的三个地区实施,项目数据收集自 2011 年 11 月至 2012 年 10 月。共有 137 名社区生殖健康代理(CBRHA)接受了提供注射类避孕药具的培训,并从一个由项目资金创建的药品循环基金中获得了 25 支注射类避孕药具的贷款。CBRHA 每为一名妇女注射一剂的收费为 3 比尔(0.17 美元),而她们向妇女提供注射服务的收费为 5 比尔(0.29 美元),这是根据支付意愿数据确定的。社会营销被用来提高认识和产生需求。采用定量和定性方法来检验干预措施的重要可行性方面。
在培训时,有 44%的 CBRHA 正在提供计划生育方法,96%的人认为提供注射类避孕药具将改善他们的服务。截至 2012 年 10 月,137 名 CBRHA 已成功完成培训并提供了 2541 次注射。在总注射次数中,47%是为新使用注射类避孕药具的妇女提供的。约 31%的注射是免费提供给最贫困的妇女,包括青少年。
该模式实施的第一年中获得的见解为在埃塞俄比亚提格雷进一步扩展提供了框架。我们的经验强调了项目规划者如何根据家庭计划偏好调整干预措施,并以更大的影响力创造更可持续的避孕药具提供。