Médecins Sans Frontières, Mumbai, India.
PLoS One. 2013 Jul 19;8(7):e68869. doi: 10.1371/journal.pone.0068869. Print 2013.
Little is known about the treatment of multidrug-resistant tuberculosis (MDR-TB) in HIV-co-infected adolescents. This study aimed to present the intermediate outcomes of HIV-infected adolescents aged 10-19 years receiving second-line anti-TB treatment in a Médecins Sans Frontières (MSF) project in Mumbai, India.
A retrospective review of medical records of 11 adolescents enrolled between July 2007 and January 2013 was undertaken. Patients were initiated on either empirical or individualized second-line ambulatory anti-TB treatment under direct observation.
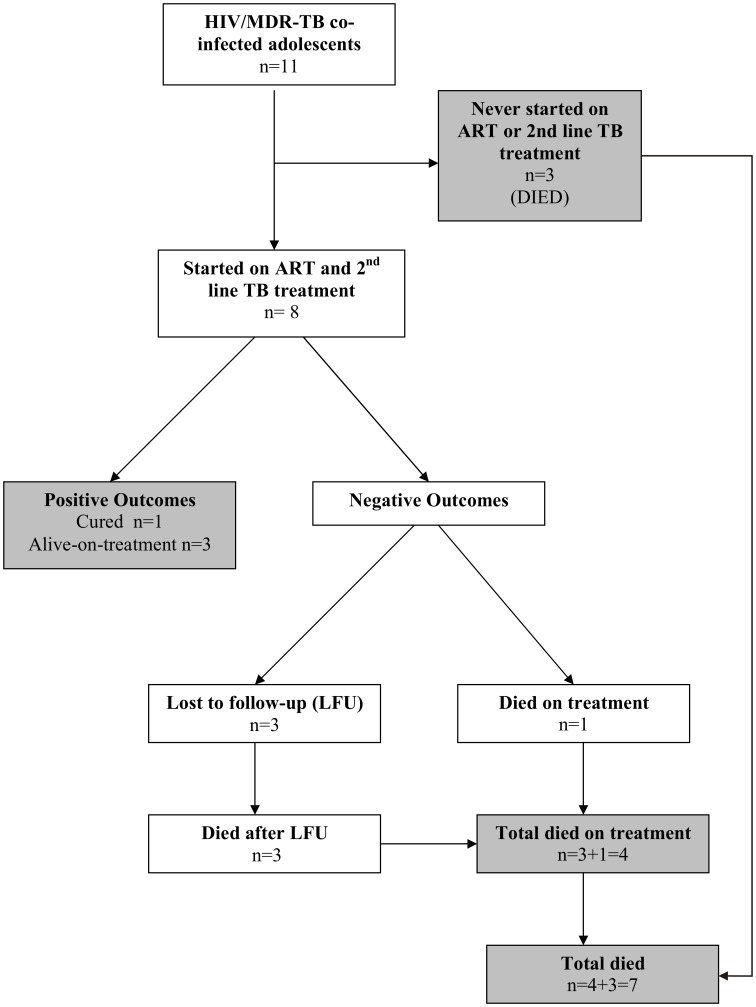
The median age was 16 (IQR 14-18) years and 54% were female. Five (46%) adolescents had pulmonary TB (PTB), two (18%) extrapulmonary disease (EPTB) and four (36%) had both. Median CD4 count at the time of MDR-TB diagnosis was 162.7 cells/µl (IQR: 84.8-250.5). By January 2013, eight patients had final and 3 had interim outcomes. Favourable results were seen in four (36.5%) patients: one was cured and three were still on treatment with negative culture results. Seven patients (64%) had poor outcomes: four (36.5%) died and three (27%) defaulted. Three of the patients who died never started on antiretroviral and/or TB treatment and one died 16 days after treatment initiation. Two of the defaulted died soon after default. All patients (100%) on-treatment experienced adverse events (AEs): two required permanent discontinuation of the culprit drug and two were hospitalized due to AEs. No patient required permanent discontinuation of the entire second-line TB or antiretroviral regimens.
Early mortality and mortality after default were the most common reasons for poor outcomes in this study. Early mortality suggests the need for rapid diagnosis and prompt treatment initiation, and adolescents might benefit from active contact-tracing and immediate referral. Default occurred at different times, suggesting the need for continuous, intensified and individualized psychosocial support for co-infected adolescents. Operational research among co-infected adolescents will be especially important in designing effective interventions for this vulnerable group.
对于合并 HIV 感染的青少年耐多药结核病(MDR-TB)的治疗,目前所知甚少。本研究旨在报告在印度孟买无国界医生组织(MSF)项目中接受二线抗结核治疗的 10-19 岁合并 HIV 感染青少年的中间结局。
对 2007 年 7 月至 2013 年 1 月期间入组的 11 例青少年患者的病历进行回顾性分析。患者接受经验性或个体化的门诊二线抗结核治疗,并在直接观察下进行。
中位年龄为 16(IQR 14-18)岁,54%为女性。5 例(46%)为肺结核(PTB),2 例(18%)为肺外疾病(EPTB),4 例(36%)两者兼有。MDR-TB 诊断时的中位 CD4 计数为 162.7 个细胞/µl(IQR:84.8-250.5)。截至 2013 年 1 月,8 例患者有最终结局,3 例有中期结局。4 例(36.5%)患者结局良好:1 例治愈,3 例仍在治疗中且培养结果为阴性。7 例(64%)患者结局较差:4 例(36.5%)死亡,3 例(27%)失访。3 例死亡的患者从未开始抗逆转录病毒和/或结核治疗,1 例在治疗开始后 16 天死亡。2 例失访的患者在失访后不久死亡。所有接受治疗的患者(100%)均发生不良事件(AE):2 例需要永久停用可疑药物,2 例因 AE 住院。无患者需要永久停用二线抗结核或抗逆转录病毒方案。
本研究中,不良结局最常见的原因是早期死亡和失访后死亡。早期死亡表明需要快速诊断和及时治疗启动,而青少年可能受益于主动接触追踪和及时转诊。失访发生在不同的时间,这表明需要持续、强化和个体化的心理社会支持,以满足合并感染的青少年的需求。针对合并感染青少年的开展运营研究对于为这一脆弱群体设计有效的干预措施尤为重要。