Doris Duke Medical Research Institute, 2nd Floor, University of KwaZulu-Natal, 719 Umbilo Road, Private Bag X7, Congella, 4013, Durban, South Africa.
Ann Intern Med. 2012 Sep 4;157(5):313-24. doi: 10.7326/0003-4819-157-5-201209040-00004.
Concerns about the immune reconstitution inflammatory syndrome (IRIS) remain a barrier to antiretroviral therapy (ART) initiation during antituberculosis treatment in co-infected patients.
To assess IRIS incidence, severity, and outcomes relative to the timing of ART initiation in patients with HIV-related tuberculosis.
Randomized, open-label clinical trial. (ClinicalTrials.gov registration number: NCT00398996)
An outpatient clinic in Durban, South Africa.
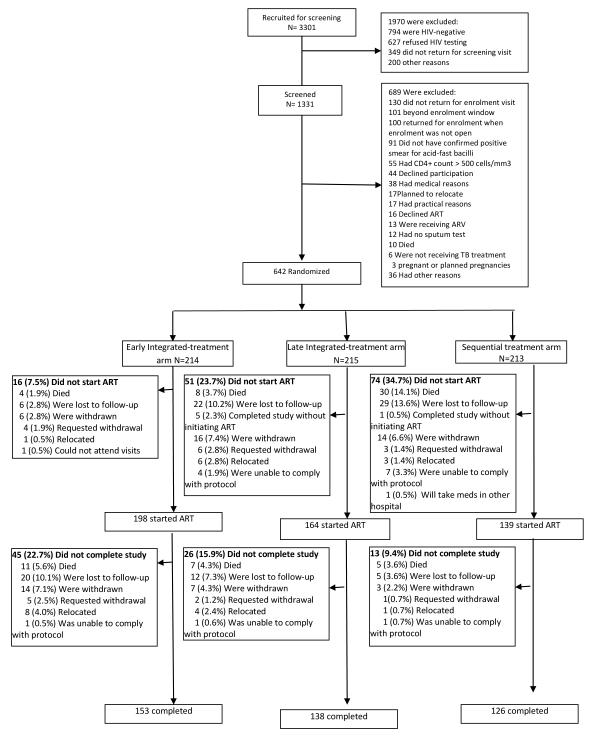
642 patients co-infected with HIV and tuberculosis.
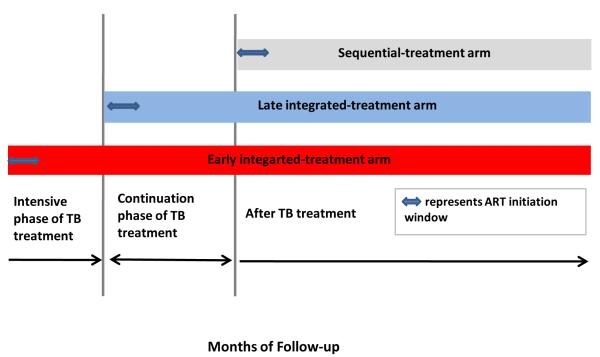
In a secondary analysis of the SAPiT (Starting Antiretroviral Therapy at Three Points in Tuberculosis) trial, IRIS was assessed in patients randomly assigned to initiate ART within 4 weeks of tuberculosis treatment initiation (early integrated treatment group), within 4 weeks of completion of the intensive phase of tuberculosis treatment (late integrated treatment group), or within 4 weeks after tuberculosis therapy completion (sequential treatment group). The syndrome was defined as new-onset or worsening symptoms, signs, or radiographic manifestations temporally related to treatment initiation, accompanied by a treatment response. Severity of IRIS, hospitalization, and time to resolution were monitored.
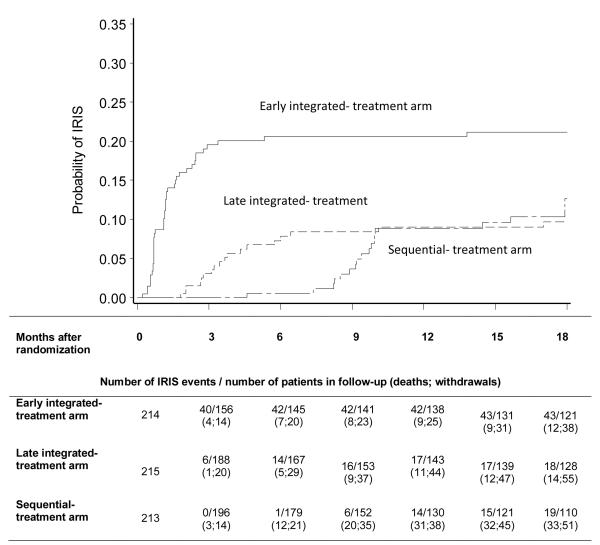
Incidence of IRIS was 19.5 (n = 43), 7.5 (n = 18), and 8.1 (n = 19) per 100 person-years in the early integrated, late integrated, and sequential treatment groups, respectively. Among patients with a baseline CD4+ count less than 0.050 × 109 cells/L, IRIS incidence was 45.5, 9.7, and 19.7 per 100 person-years in the early integrated, late integrated, and sequential treatment groups, respectively. Incidence of IRIS was higher in the early integrated treatment group than in the late integrated (incidence rate ratio, 2.6 [95% CI, 1.5 to 4.8]; P < 0.001) or sequential (incidence rate ratio, 2.4 [CI, 1.4 to 4.4]; P < 0.001) treatment groups. More severe IRIS cases occurred in the early integrated treatment group than in the other 2 groups (35% vs. 19%; P = 0.179), and patients in the early integrated treatment group had significantly higher hospitalization rates (42% vs. 14%; P = 0.007) and longer time to resolution (70.5 vs. 29.0 days; P = 0.001) than patients in the other 2 groups.
It was not possible to assess IRIS in more patients in the sequential treatment group (n = 74) than in the late integrated (n = 50) and early integrated (n = 32) treatment groups because of loss to follow-up, withdrawal, or death within 6 months of scheduled ART initiation. This study did not assess IRIS risk in nonambulatory patients or in those with extrapulmonary and smear-negative tuberculosis.
Initiation of ART in early stages of tuberculosis treatment resulted in significantly higher IRIS rates, longer time to resolution, and more severe cases of IRIS requiring hospitalization. These findings are particularly relevant to patients initiating ART with a CD4+ count less than 0.050 × 109 cells/L, given the increased survival benefit of early ART initiation in this group.
Comprehensive International Program of Research on AIDS.
在合并感染患者中,抗逆转录病毒治疗(ART)启动时对免疫重建炎症综合征(IRIS)的担忧仍然是一个障碍。
评估与 HIV 相关结核病患者中 ART 启动时间相关的 IRIS 发生率、严重程度和结局。
随机、开放标签临床试验。(临床试验.gov 注册号:NCT00398996)
南非德班的一个门诊诊所。
642 例合并 HIV 和结核病的患者。
在 SAPiT(结核病治疗开始时三点开始抗逆转录病毒治疗)试验的二次分析中,根据随机分配在开始结核病治疗后 4 周内(早期综合治疗组)、完成结核病强化期治疗后 4 周内(晚期综合治疗组)或在结核病治疗完成后 4 周内(序贯治疗组)启动 ART 的患者评估 IRIS。该综合征被定义为新出现或恶化的症状、体征或影像学表现与治疗开始时间有关,伴有治疗反应。监测 IRIS 的严重程度、住院治疗和恢复时间。
早期综合、晚期综合和序贯治疗组的 IRIS 发生率分别为每 100 人年 19.5(n = 43)、7.5(n = 18)和 8.1(n = 19)。在基线 CD4+计数小于 0.050×109 个细胞/L 的患者中,早期综合、晚期综合和序贯治疗组的 IRIS 发生率分别为每 100 人年 45.5、9.7 和 19.7。早期综合治疗组的 IRIS 发生率高于晚期综合(发病率比,2.6[95%CI,1.5 至 4.8];P<0.001)或序贯(发病率比,2.4[CI,1.4 至 4.4];P<0.001)治疗组。早期综合治疗组发生更严重的 IRIS 病例多于其他两组(35%比 19%;P=0.179),早期综合治疗组的住院率(42%比 14%;P=0.007)和恢复时间(70.5 比 29.0 天;P=0.001)也显著高于其他两组。
由于失访、退出或在计划开始 ART 后 6 个月内死亡,无法在序贯治疗组(n = 74)中评估更多患者的 IRIS,而在晚期综合治疗组(n = 50)和早期综合治疗组(n = 32)中可以评估。本研究未评估非卧床患者或肺外和涂片阴性结核病患者的 IRIS 风险。
在结核病治疗的早期阶段启动 ART 会导致更高的 IRIS 发生率、更长的恢复时间以及更严重的需要住院治疗的 IRIS 病例。对于 CD4+计数小于 0.050×109 个细胞/L 的患者开始 ART 时,这些发现尤为重要,因为在该组中早期 ART 启动可显著提高生存获益。
国际艾滋病综合研究计划。