Division of Cardiovascular Medicine, Brigham and Women's Hospital, Boston, MA, USA.
Am Heart J. 2013 Aug;166(2):199-207.e15. doi: 10.1016/j.ahj.2013.03.018. Epub 2013 May 3.
Inflammation plays a fundamental role in atherothrombosis. Yet, whether direct inhibition of inflammation will reduce the occurrence of adverse cardiovascular outcomes is not known.
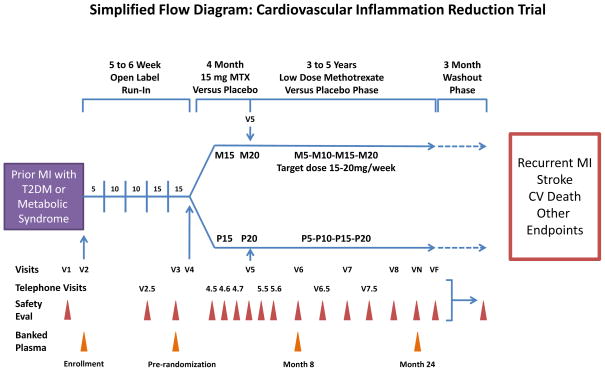
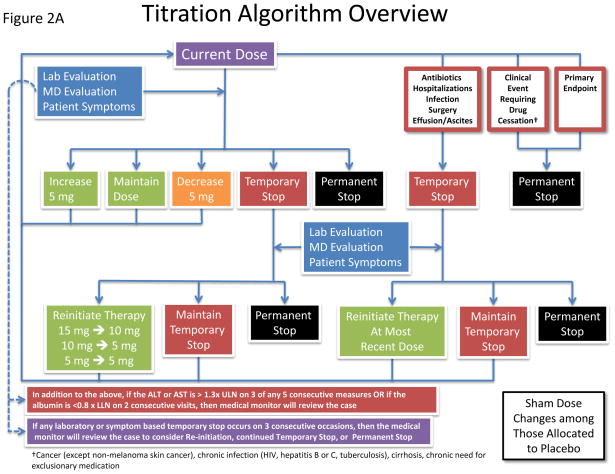
The Cardiovascular Inflammation Reduction Trial (CIRT) (ClinicalTrials.govNCT01594333) will randomly allocate 7,000 patients with prior myocardial infarction (MI) and either type 2 diabetes or the metabolic syndrome to low-dose methotrexate (target dose 15-20 mg/wk) or placebo over an average follow-up period of 3 to 5 years. Low-dose methotrexate is a commonly used anti-inflammatory regimen for the treatment of rheumatoid arthritis and lacks significant effects on lipid levels, blood pressure, or platelet function. Both observational and mechanistic studies suggest that low-dose methotrexate has clinically relevant antiatherothrombotic effects. The CIRT primary end point is a composite of nonfatal MI, nonfatal stroke, and cardiovascular death. Secondary end points are all-cause mortality, coronary revascularization plus the primary end point, hospitalization for congestive heart failure plus the primary end point, all-cause mortality plus coronary revascularization plus congestive heart failure plus the primary end point, incident type 2 diabetes, and net clinical benefit or harm. CIRT will use standardized central methodology designed to ensure consistent performance of all dose adjustments and safety interventions at each clinical site in a manner that protects the blinding to treatment but maintains safety for enrolled participants.
CIRT aims to test the inflammatory hypothesis of atherothrombosis in patients with prior MI and either type 2 diabetes or metabolic syndrome, conditions associated with persistent inflammation. If low-dose methotrexate reduces cardiovascular events, CIRT would provide a novel therapeutic approach for the secondary prevention of heart attack, stroke, and cardiovascular death.
炎症在动脉粥样硬化血栓形成中起着根本性的作用。然而,直接抑制炎症是否会减少不良心血管结局的发生尚不清楚。
心血管炎症减少试验(CIRT)(ClinicalTrials.govNCT01594333)将随机分配 7000 名既往心肌梗死(MI)且患有 2 型糖尿病或代谢综合征的患者接受低剂量甲氨蝶呤(目标剂量 15-20mg/周)或安慰剂治疗,平均随访时间为 3 至 5 年。低剂量甲氨蝶呤是一种常用于治疗类风湿关节炎的抗炎方案,对血脂水平、血压或血小板功能没有显著影响。观察性和机制研究均表明,低剂量甲氨蝶呤具有临床相关的抗动脉粥样硬化血栓形成作用。CIRT 的主要终点是复合的非致死性心肌梗死、非致死性卒中和心血管死亡。次要终点是全因死亡率、冠状动脉血运重建加上主要终点、充血性心力衰竭住院加上主要终点、全因死亡率加上冠状动脉血运重建加上充血性心力衰竭加上主要终点、新发 2 型糖尿病以及净临床获益或危害。CIRT 将采用标准化的中心方法,旨在确保在每个临床站点以保护治疗盲法的方式一致地进行所有剂量调整和安全干预,同时为入组参与者提供安全性。
CIRT 旨在检验既往有 MI 且患有 2 型糖尿病或代谢综合征的患者的动脉粥样硬化血栓形成的炎症假说,这些情况与持续存在的炎症有关。如果低剂量甲氨蝶呤减少心血管事件,CIRT 将为心脏病发作、卒中和心血管死亡的二级预防提供一种新的治疗方法。