Westphal Glauco Adrieno, Zaclikevis Viviane Renata, Vieira Kalinca Daberkow, Cordeiro Rodrigo de Brito, Horner Marina Borges W, Oliveira Thamy Pellizzaro de, Duarte Robson, Sperotto Geonice, Silveira Georgiana da, Caldeira Filho Milton, Coll Elisabeth, Yus-Teruel Santiago
Centro Hospitalar Unimed - CHU - Joinville (SC), Brazil.
Rev Bras Ter Intensiva. 2012 Dec;24(4):334-40. doi: 10.1590/s0103-507x2012000400007.
To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals.
A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student's t- and chi-square tests were used, and p-value < 0.05 was considered to be significant.
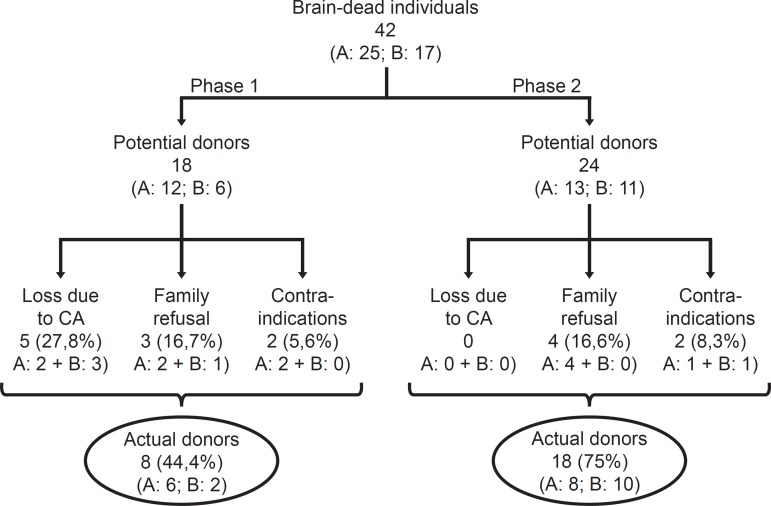
A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary.
The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
评估在两家医院应用一种管理方案对已故潜在多器官捐赠者进行维持性护理的效果。
在两家综合医院进行一项前后对照(第1阶段/第2阶段)研究,纳入连续入住两个重症监护病房的潜在捐赠者。在第1阶段(16个月),回顾性收集数据,潜在捐赠者的维持性护理措施由重症监护医生制定。在第2阶段(12个月),前瞻性收集数据,并使用一种管理方案进行维持性护理。比较两个阶段的人口统计学变量、脑死亡诊断时及过程结束时的生理变量、脑死亡确认试验及过程结束的执行时间、对维持性护理基本措施集束的依从性、心脏骤停导致的损失、家属拒绝、禁忌症以及潜在捐赠者转化为实际捐赠者的转化率。采用学生t检验和卡方检验,p值<0.05被认为具有统计学意义。
共识别出42名潜在捐赠者(第1阶段18名,第2阶段24名)。第2阶段首次临床评估至恢复的时间间隔缩短(第1阶段:35.0±15.5小时 vs 第2阶段:24.6±6.2小时;p = 0.023)。维持性护理19项基本项目中的依从性提高至10项,第2阶段心脏骤停导致的损失也有所减少(第1阶段:27.8% vs 第2阶段:0%;p = 0.006),而转化率有所提高(第1阶段:44.4% vs 第2阶段:75%;p = 0.044)。家属拒绝和医学禁忌症导致的损失没有变化。
采用侧重于对潜在已故捐赠者进行护理的基本措施应用的管理方案,可能会减少因心脏骤停导致的潜在捐赠者损失。