Department of Nephrology, University Hospitals Coventry and Warwickshire National Health Service Trust, Coventry, United Kingdom.
PLoS One. 2013 Jul 26;8(7):e68663. doi: 10.1371/journal.pone.0068663. Print 2013.
HLA directed antibodies play an important role in acute and chronic allograft rejection. During viral infection of a patient with HLA antibodies, the HLA antibody levels may rise even though there is no new immunization with antigen. However it is not known whether the converse occurs, and whether changes on non-donor specific antibodies are associated with any outcomes following HLA antibody incompatible renal transplantation.
55 patients, 31 women and 24 men, who underwent HLAi renal transplant in our center from September 2005 to September 2010 were included in the studies. We analysed the data using two different approaches, based on; i) DSA levels and ii) rejection episode post transplant. HLA antibody levels were measured during the early post transplant period and corresponding CMV, VZV and Anti-HBs IgG antibody levels and blood group IgG, IgM and IgA antibodies were quantified.
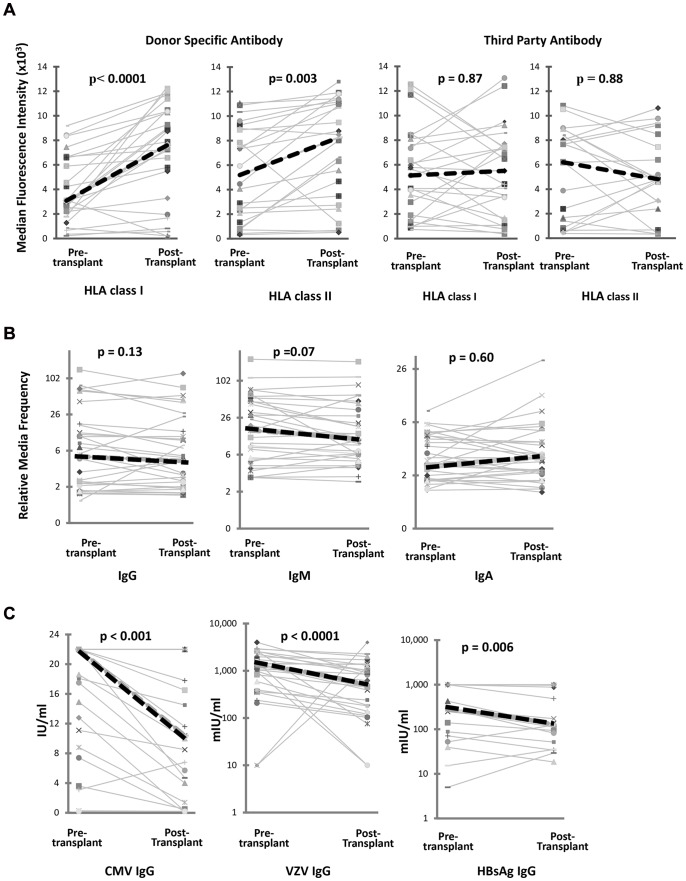
Despite a significant DSA antibody rise no significant non-donor specific HLA antibody, viral or blood group antibody rise was found. In rejection episode analyses, multiple logistic regression modelling showed that change in the DSA was significantly associated with rejection (p = 0.002), even when adjusted for other antibody levels. No other antibody levels were predictive of rejection. Increase in DSA from pre treatment to a post transplant peak of 1000 was equivalent to an increased chance of rejection with an odds ratio of 1.47 (1.08, 2.00).
In spite of increases or decreases in the DSA levels, there were no changes in the viral or the blood group antibodies in these patients. Thus the DSA rise is specific in contrast to the viral, blood group or third party antibodies post transplantation. Increases in the DSA post transplant in comparison to pre-treatment are strongly associated with occurrence of rejection.
HLA 定向抗体在急性和慢性同种异体移植物排斥反应中起着重要作用。在具有 HLA 抗体的患者发生病毒感染时,即使没有新的抗原免疫,HLA 抗体水平也可能升高。然而,目前尚不清楚是否会出现相反的情况,以及非供体特异性抗体的变化是否与 HLA 抗体不相容的肾移植后任何结果相关。
本研究纳入了 2005 年 9 月至 2010 年 9 月在我们中心接受 HLAi 肾移植的 55 例患者,其中 31 例为女性,24 例为男性。我们使用两种不同的方法分析了数据,一种基于;i)DSA 水平和 ii)移植后排斥反应。在移植后的早期阶段测量了 HLA 抗体水平,并定量了相应的 CMV、VZV 和抗-HBs IgG 抗体以及血型 IgG、IgM 和 IgA 抗体。
尽管 DSA 抗体明显升高,但未发现非供体特异性 HLA 抗体、病毒或血型抗体明显升高。在排斥反应分析中,多变量逻辑回归模型显示,DSA 的变化与排斥反应显著相关(p = 0.002),即使在调整了其他抗体水平后也是如此。没有其他抗体水平可预测排斥反应。DSA 从治疗前增加到移植后峰值 1000 等效于排斥反应的机会增加,优势比为 1.47(1.08,2.00)。
尽管 DSA 水平升高或降低,但这些患者的病毒或血型抗体没有变化。因此,与移植后病毒、血型或第三方抗体相比,DSA 升高具有特异性。与治疗前相比,移植后 DSA 的增加与排斥反应的发生强烈相关。