School of Biomedical Engineering, Capital Medical University, Beijing, People's Republic of China.
Neuropsychiatr Dis Treat. 2013;9:1003-10. doi: 10.2147/NDT.S47099. Epub 2013 Jul 26.
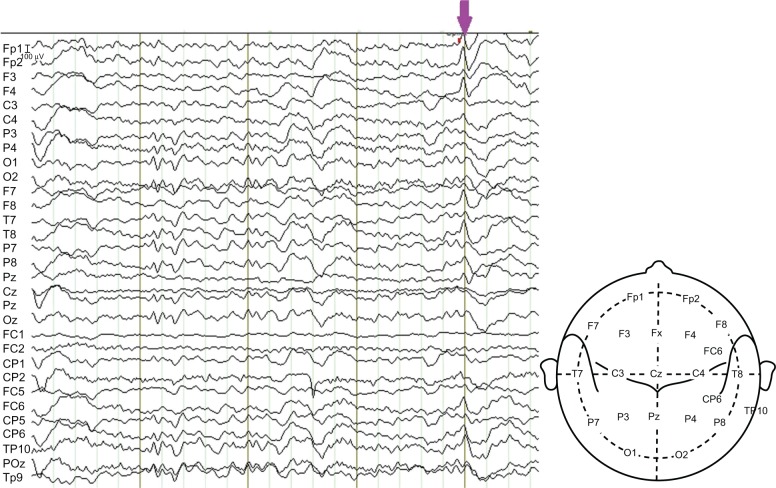
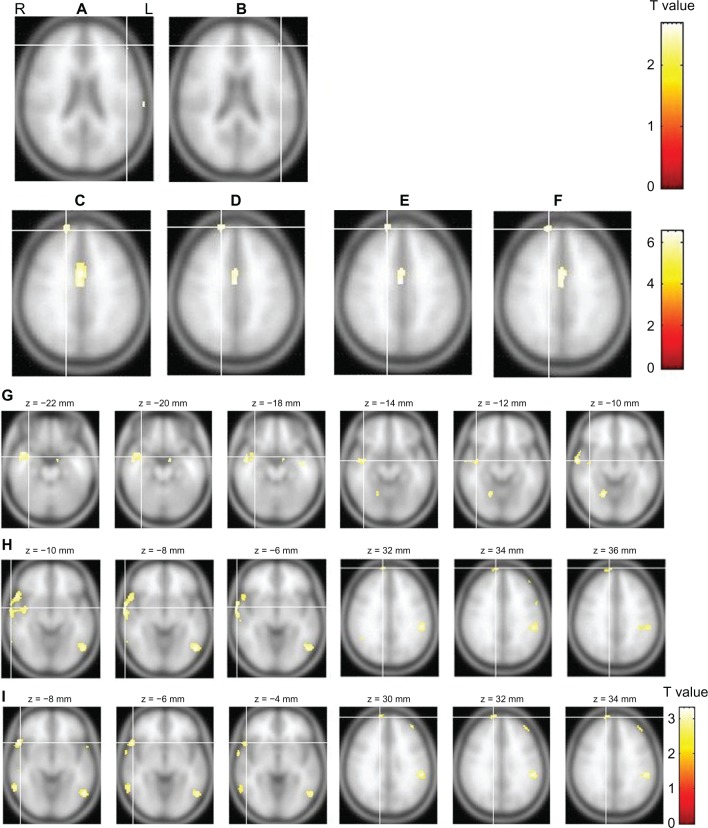
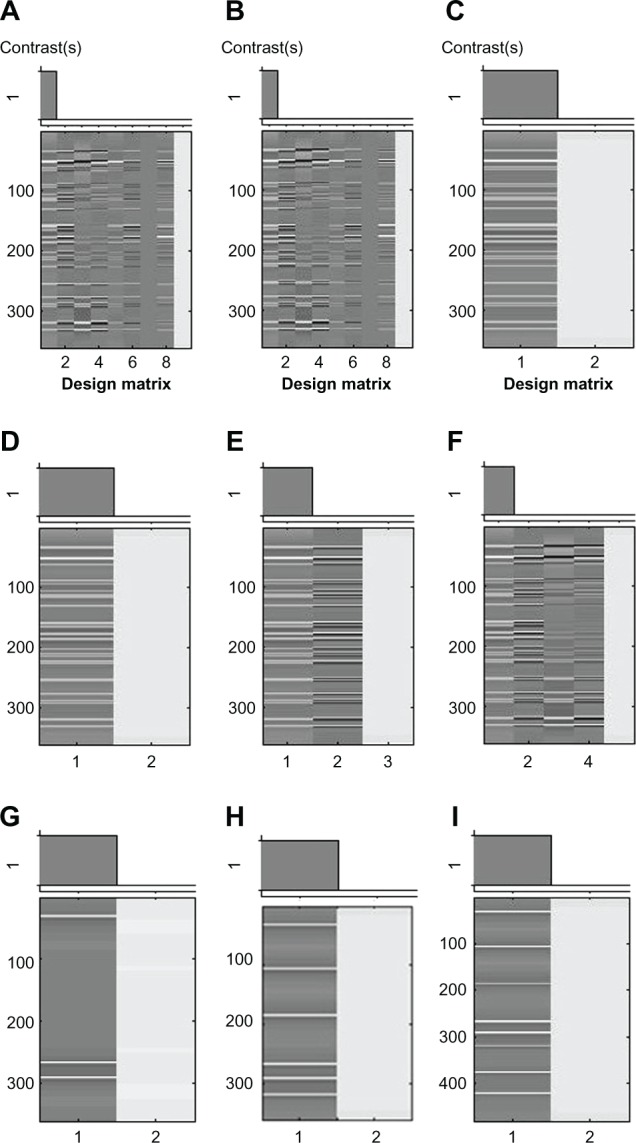
Epilepsy surgery has improved over the last decade, but non-seizure-free outcome remains at 10%-40% in temporal lobe epilepsy (TLE) and 40%-60% in extratemporal lobe epilepsy (ETLE). This paper reports a complex multifocal case. With a normal magnetic resonance imaging (MRI) result and nonlocalizing electroencephalography (EEG) findings (bilateral TLE and ETLE, with more interictal epileptiform discharges [IEDs] in the right frontal and temporal regions), a presurgical EEG-functional MRI (fMRI) was performed before the intraoperative intracranial EEG (icEEG) monitoring (icEEG with right hemispheric coverage). Our previous EEG-fMRI analysis results (IEDs in the left hemisphere alone) were contradictory to the EEG and icEEG findings (IEDs in the right frontal and temporal regions). Thus, the EEG-fMRI data were reanalyzed with newly identified IED onsets and different fMRI model options. The reanalyzed EEG-fMRI findings were largely concordant with those of EEG and icEEG, and the failure of our previous EEG-fMRI analysis may lie in the inaccurate identification of IEDs and wrong usage of model options. The right frontal and temporal regions were resected in surgery, and dual pathology (hippocampus sclerosis and focal cortical dysplasia in the extrahippocampal region) was found. The patient became seizure-free for 3 months, but his seizures restarted after antiepileptic drugs (AEDs) were stopped. The seizures were not well controlled after resuming AEDs. Postsurgical EEGs indicated that ictal spikes in the right frontal and temporal regions reduced, while those in the left hemisphere became prominent. This case suggested that (1) EEG-fMRI is valuable in presurgical evaluation, but requires caution; and (2) the intact seizure focus in the remaining brain may cause the non-seizure-free outcome.
癫痫手术在过去十年中有所改进,但颞叶癫痫(TLE)的无发作结果仍为 10%-40%,而外侧颞叶癫痫(ETLE)的无发作结果为 40%-60%。本文报告了一个复杂的多灶性病例。患者磁共振成像(MRI)结果正常,脑电图(EEG)无定位发现(双侧 TLE 和 ETLE,右侧额颞区有更多的发作间期癫痫样放电[IEDs]),在术中颅内脑电图(icEEG)监测(右侧半球覆盖的 icEEG)前进行了术前 EEG-功能磁共振成像(fMRI)。我们之前的 EEG-fMRI 分析结果(仅左半球有 IEDs)与 EEG 和 icEEG 结果(右侧额颞区的 IEDs)相矛盾。因此,使用新确定的 IED 发作和不同的 fMRI 模型选项重新分析 EEG-fMRI 数据。重新分析的 EEG-fMRI 结果与 EEG 和 icEEG 的结果基本一致,我们之前的 EEG-fMRI 分析失败可能在于 IEDs 的不准确识别和模型选项的错误使用。手术中切除了右侧额颞区,发现存在双重病变(海马硬化和海马旁区局灶性皮质发育不良)。患者术后 3 个月无发作,但停药后癫痫发作再次发作。重新开始使用 AEDs 后,癫痫发作仍未得到很好的控制。术后 EEG 显示右侧额颞区的发作棘波减少,而左侧半球的发作棘波变得明显。该病例表明:(1)EEG-fMRI 对术前评估很有价值,但需要谨慎;(2)残留大脑中完整的癫痫灶可能导致无发作结果。