Moradi Ghobad, Mohammad Kazem, Majdzadeh Reza, Ardakani Hossein Malekafzali, Naieni Kourosh Holakouie
Epidemiology and Biostatistics Department, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran.
Int J Prev Med. 2013 Jun;4(6):671-83.
The most fundamental way to decrease the burden of noncommunicable diseases (NCDs) is to identify and control their related risk factors. The goal of this study is to determine socioeconomic inequalities in risk factors for NCDs using concentration index based on Non-Communicable Disease Surveillance Survey (NCDSS) data in Kurdistan province, Islamic Republic of Iran in 2005 and 2009.
The required data for this study are taken from two NCDSSs in Kurdistan province in 2005 and 2009. A total of 2,494 persons in 2005 and 997 persons in 2009 were assessed. Concentration index was used to determine socioeconomic inequality. To assess the relationship between the prevalence of each risk factor and socioeconomic status (SES), logistic regression was used and odds ratio (OR) was calculated for each group, compared with the poorest group.
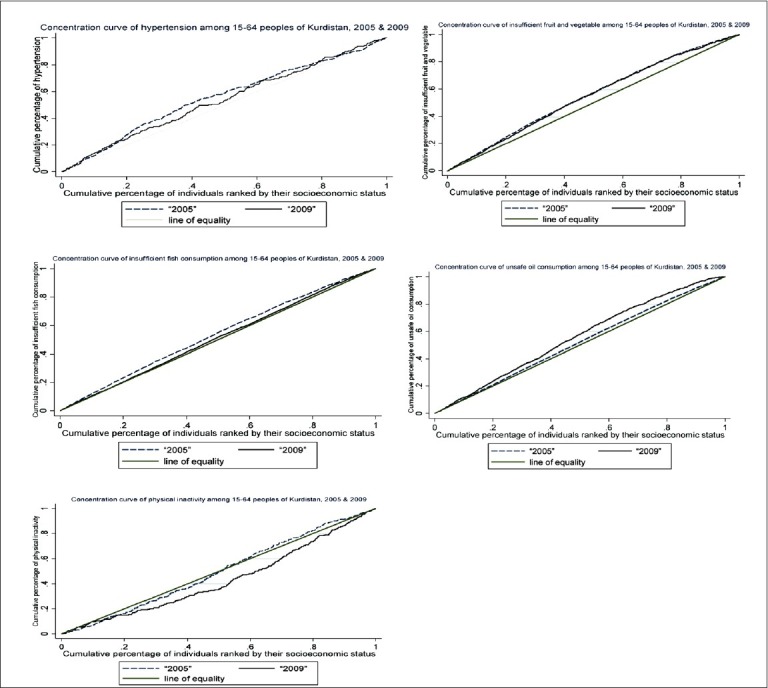
The concentration index for hypertension was -0.095 (-0.158, -0.032) in 2005 and -0.080 (-0.156, -0.003) in 2009. The concentration index for insufficient consumption of fruits and vegetables was -0.117 (-0.153, -0.082) in 2005 and -0.100 (-0.153, -0.082) in 2009. The concentration index for the consumption of unhealthy fat and oil was -0.034 (-0.049, -0.019) in 2005 and -0.108 (-0.165, -0.051) in 2009. The concentration index for insufficient consumption of fish was -0.070 (-0.096, -0.044) in 2005. The concentration index for physical inactivity was 0.008 (-0.057, 0.075) in 2005 and 0.139 (0.063, 0.215) in 2009. In all the cases, the OR of the richest group to the poorest group was significant.
Hypertension, insufficient consumption of fruits and vegetables, consumption of unhealthy fat and oil, and insufficient consumption of fish are more prevalent among poor groups. There was no significant socioeconomic inequality in the distribution of smoking, excess weight, and hypercholesterolemia. Physical inactivity was more prevalent among the rich groups of society in 2009. The reduction of socioeconomic inequalities must become a main goal in health-care policies.
减轻非传染性疾病(NCDs)负担的最根本方法是识别并控制其相关风险因素。本研究的目的是利用基于伊朗伊斯兰共和国库尔德斯坦省2005年和2009年非传染性疾病监测调查(NCDSS)数据的浓度指数,确定非传染性疾病风险因素中的社会经济不平等情况。
本研究所需数据取自库尔德斯坦省2005年和2009年的两次NCDSS。2005年共评估了2494人,2009年评估了997人。使用浓度指数来确定社会经济不平等情况。为评估每个风险因素的患病率与社会经济地位(SES)之间的关系,采用逻辑回归,并计算每组与最贫困组相比的优势比(OR)。
2005年高血压的浓度指数为-0.095(-0.158,-0.032),2009年为-0.080(-0.156,-0.003)。2005年水果和蔬菜摄入不足的浓度指数为-0.117(-0.153,-0.082),2009年为-0.100(-0.153,-0.082)。2005年不健康脂肪和油类消费的浓度指数为-0.034(-0.049,-0.019),2009年为-0.108(-0.165,-0.051)。2005年鱼类摄入不足的浓度指数为-0.070(-0.096,-0.044)。2005年身体活动不足的浓度指数为0.008(-0.057,0.075),2009年为0.139(0.063,0.215)。在所有情况下,最富有组与最贫困组的OR均具有显著性。
高血压、水果和蔬菜摄入不足、不健康脂肪和油类消费以及鱼类摄入不足在贫困群体中更为普遍。吸烟、超重和高胆固醇血症的分布不存在显著的社会经济不平等。2009年身体活动不足在社会富裕群体中更为普遍。减少社会经济不平等必须成为医疗保健政策的主要目标。