Department of Clinical Microbiology, Aalborg University Hospital, Aalborg, Denmark.
PLoS One. 2013 Jul 25;8(7):e70082. doi: 10.1371/journal.pone.0070082. Print 2013.
To examine the effect of socioeconomic status (SES) on mortality in patients with bacteremia and the underlying factors that may mediate differences in mortality.
We conducted a population-based cohort study in two Danish regions. All patients 30 to 65 years of age with first time bacteremia from 2000 through 2008 were identified in a population-based microbiological bacteremia database (n = 8,653). Individual-level data on patients' SES (educational level and personal income) and comorbid conditions were obtained from public and medical registries. We used Cox regression to examine mortality within 30 days after bacteremia with and without cumulative adjustment for potential mediators.
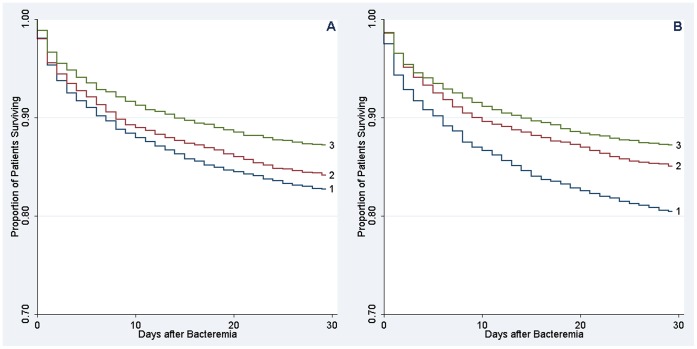
Bacteremia patients of low SES were more likely to live alone and be unmarried than patients of high SES. They also had more pre-existing comorbidity, more substance abuse, more Staphylococcus aureus and nosocomial infections, and more admissions to small nonteaching hospitals. Overall, 1,374 patients (15.9%) died within 30 days of follow-up. Patients of low SES had consistently higher mortality after bacteremia than those of high SES crude hazard ratio for low vs. high education, 1.38 [95% confidence interval (CI), 1.18-1.61]; crude hazard ratio for low-income vs. high-income tertile, 1.58 [CI, 1.39-1.80]. Adjustment for differences in social support, pre-existing comorbidity, substance abuse, place of acquisition of the infection, and microbial agent substantially attenuated the effect of SES on mortality (adjusted hazard ratio for low vs. high education, 1.15 [95% CI, 0.98-1.36]; adjusted hazard ratio for low-income vs. high-income tertile, 1.29 [CI, 1.12-1.49]). Further adjustment for characteristics of the admitting hospital had minimal effect on observed mortality differences.
Low SES was strongly associated with increased 30-day mortality after bacteremia. Less social support, more pre-existing comorbidity, more substance abuse, and differences in place of acquisition and agent of infection appeared to mediate much of the observed disparities in mortality.
研究社会经济地位(SES)对菌血症患者死亡率的影响,以及可能导致死亡率差异的潜在因素。
我们在丹麦的两个地区进行了一项基于人群的队列研究。从 2000 年至 2008 年,从一个基于人群的微生物菌血症数据库中确定了 30 至 65 岁首次发生菌血症的所有患者(n=8653)。从公共和医疗登记处获得了患者 SES(教育水平和个人收入)和合并症的个体水平数据。我们使用 Cox 回归分析了菌血症后 30 天内的死亡率,包括在累积调整潜在中介因素后。
低 SES 的菌血症患者比高 SES 的患者更有可能独居和未婚。他们也有更多的预先存在的合并症、更多的药物滥用、更多的金黄色葡萄球菌和医院感染,以及更多的小非教学医院入院。总的来说,8653 名患者中有 1374 名(15.9%)在随访 30 天内死亡。与 SES 较高的患者相比,SES 较低的患者菌血症后死亡率始终较高,低 SES 与高 SES 的粗死亡率比为 1.38(95%置信区间[CI],1.18-1.61);低 SES 与高 SES 的低收入组相比,粗死亡率比为 1.58(CI,1.39-1.80)。调整社会支持、预先存在的合并症、药物滥用、感染部位和微生物制剂方面的差异后,SES 对死亡率的影响明显减弱(低 SES 与高 SES 的调整死亡率比为 1.15(95%CI,0.98-1.36);低 SES 与高 SES 的低收入组相比,调整死亡率比为 1.29(CI,1.12-1.49))。进一步调整入院医院的特征对观察到的死亡率差异影响不大。
低 SES 与菌血症后 30 天死亡率增加密切相关。社会支持较少、预先存在的合并症较多、药物滥用较多以及感染部位和病原体的差异似乎在很大程度上解释了观察到的死亡率差异。