Department of Obstetrics and Gynaecology, University of Auckland, Auckland, New Zealand.
PLoS One. 2013 Aug 5;8(8):e70917. doi: 10.1371/journal.pone.0070917. Print 2013.
Small for gestational age (SGA) infants comprise up to 50% of all stillbirths and a minority are detected before birth. We aimed to develop and validate early pregnancy predictive models for SGA infants.
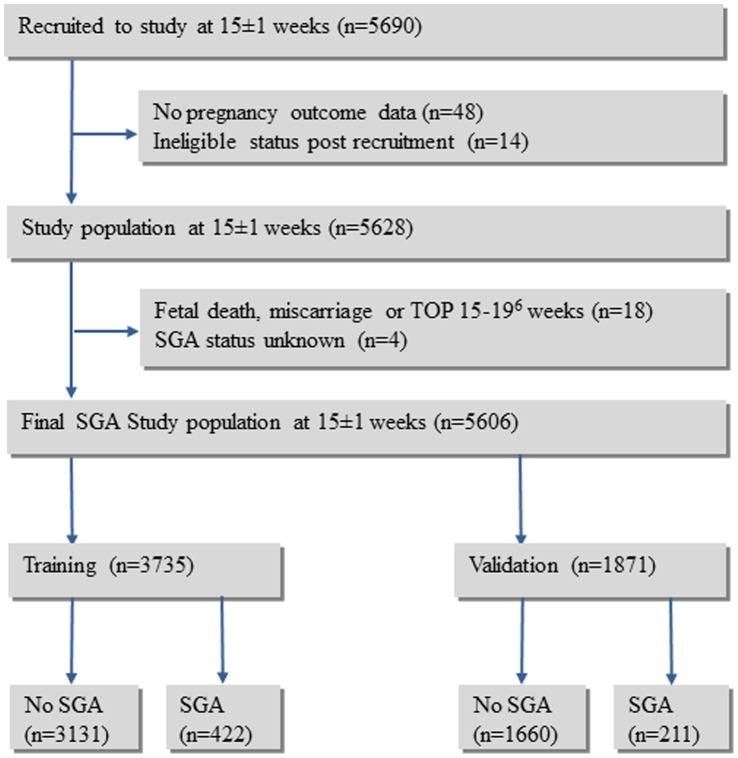
5628 participants from SCOPE, a prospective study of nulliparous pregnant women, were interviewed at 15 ± 1 weeks' gestation. Fetal anthropometry, uterine and umbilical Doppler studies were performed at 20 ± 1 weeks'. The cohort was divided into training (n = 3735) and validation datasets (n = 1871). All-SGA (birthweight <10th customised centile), Normotensive-SGA (SGA with normotensive mother) and Hypertensive-SGA (SGA with mother who developed hypertension) were the primary outcomes. Multivariable analysis was performed using stepwise logistic regression firstly using clinical variables and then with clinical and ultrasound variables. Receiver operator curves were constructed and areas under the curve (AUC) calculated.
633 infants (11.3%) in the whole cohort were SGA; 465 (8.3%) Normotensive-SGA and 165 (3.0%) Hypertensive-SGA. In the training dataset risk factors for All-SGA at 15 ± 1 weeks' included: family history of coronary heart disease, maternal birthweight <3000 g and 3000 g to 3499 g compared with ≥ 3500 g, >12 months to conceive, university student, cigarette smoking, proteinuria, daily vigorous exercise and diastolic blood pressure ≥ 80. Recreational walking ≥ 4 times weekly, rhesus negative blood group and increasing random glucose were protective. AUC for clinical risk factors was 0.63. Fetal abdominal or head circumference z scores <10(th) centile and increasing uterine artery Doppler resistance at 20 ± 1 weeks' were associated with increased risk. Addition of these parameters increased the AUC to 0.69. Clinical predictors of Normotensive and Hypertensive-SGA were sub-groups of All-SGA predictors and were quite different. The combined clinical and ultrasound AUC for Normotensive and Hypertensive-SGA were 0.69 and 0.82 respectively.
Predictors for SGA of relevance to clinical practice were identified. The identity and predictive potential differed in normotensive women and those who developed hypertension.
胎儿生长受限(SGA)婴儿占所有死胎的 50%左右,其中少数在产前即可被发现。本研究旨在建立并验证预测 SGA 婴儿的早孕期预测模型。
SCOPE 是一项前瞻性的初产妇研究,共纳入 5628 名参与者,在妊娠 15±1 周时进行访谈。在妊娠 20±1 周时进行胎儿体格测量、子宫和脐带动脉多普勒检查。将队列分为训练数据集(n=3735)和验证数据集(n=1871)。所有 SGA(出生体重<第 10 定制百分位数)、正常血压 SGA(母亲血压正常的 SGA)和高血压 SGA(母亲出现高血压的 SGA)是主要结局。首先使用逐步逻辑回归对临床变量进行多变量分析,然后使用临床和超声变量进行分析。构建受试者工作特征曲线并计算曲线下面积(AUC)。
整个队列中共有 633 名(11.3%)婴儿为 SGA;其中 465 名(8.3%)为正常血压 SGA,165 名(3.0%)为高血压 SGA。在训练数据集中,15±1 周时发生所有 SGA 的危险因素包括:家族性冠心病病史、母亲出生体重<3000 g 和 3000 g 至 3499 g 与≥3500 g、>12 个月受孕、大学生、吸烟、蛋白尿、每日剧烈运动和舒张压≥80 mmHg。每周至少进行 4 次休闲步行、Rh 阴性血和随机血糖增加是保护性因素。临床危险因素的 AUC 为 0.63。妊娠 20±1 周时胎儿腹围或头围 Z 评分<第 10 百分位数和子宫动脉多普勒阻力增加与风险增加相关。增加这些参数后,AUC 增加至 0.69。正常血压 SGA 和高血压 SGA 的临床预测因素是所有 SGA 预测因素的亚组,且两者有较大差异。正常血压 SGA 和高血压 SGA 的临床和超声联合 AUC 分别为 0.69 和 0.82。
确定了与临床实践相关的 SGA 预测因素。在正常血压的女性和出现高血压的女性中,这些因素的特征和预测潜能不同。