Health Outcomes Practice, Kantar Health, New York, New York, United States of America.
PLoS One. 2013 Aug 12;8(8):e71264. doi: 10.1371/journal.pone.0071264. eCollection 2013.
This study builds upon current studies of atrial fibrillation (AF) and health outcomes by examining more comprehensively the humanistic burden of illness (quality of life, activity impairment, and healthcare resource utilization) among adult patients with AF, using a large, nationally representative sample and matched controls.
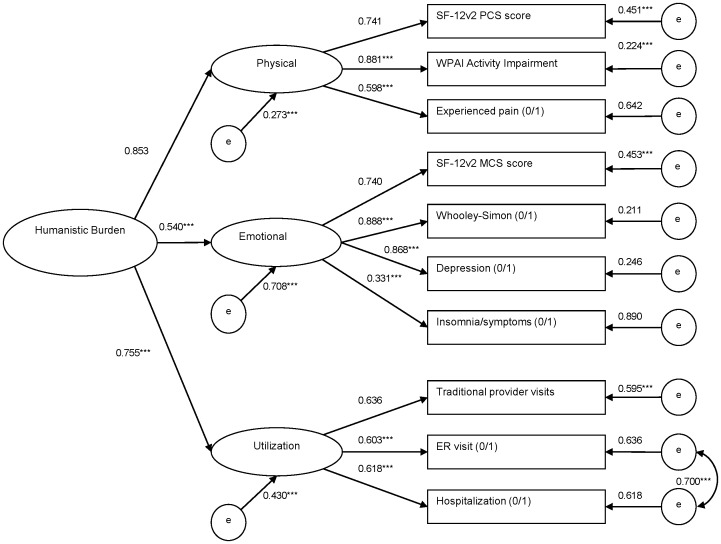
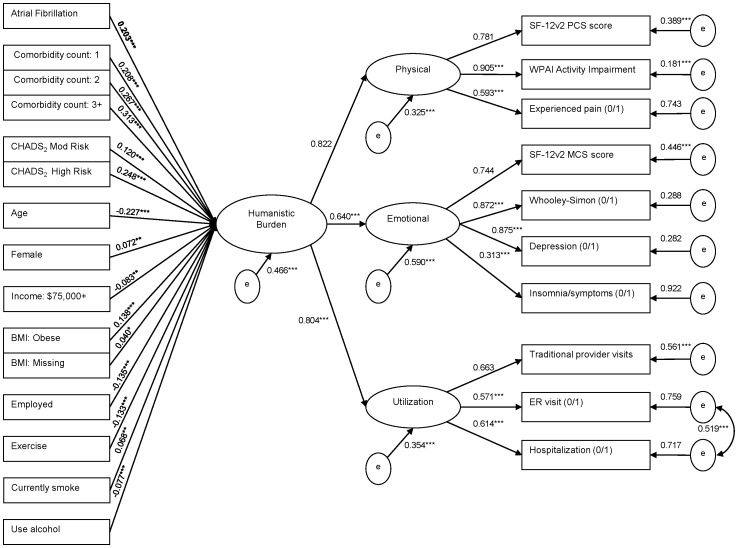
Data were analyzed from the Internet-based 2009 US National Health and Wellness Survey. Outcomes were Mental and Physical Component Summary (MCS and PCS) and health utility scores from the SF-12, activity impairment, hospitalizations, and healthcare provider and emergency room (ER) visits. Patients with self-reported diagnosis of AF were matched randomly on age and gender with an equal number of respondents without AF. Generalized linear models examined outcomes as a function of AF vs. non-AF status, controlling for CHADS2 score, comorbidity counts, demographics, and clinical variables. Exploratory structural equation modeling assessed the above in an integrated model of humanistic burden.
Mean age of AF patients (1,296 from a total sample of 75,000) was 64.9 years and 65.1% were male. Adjusting for covariates, compared with non-AF patients, AF patients had lower MCS, PCS, and utility scores, greater activity impairment (rate ratio = 1.26), more traditional provider visits (rate ratio = 1.43), and increased odds of ER visits (OR = 2.53) and hospitalizations (OR = 2.71). Exploratory structural equation modeling analyses revealed that persons with AF experienced a significantly higher overall humanistic burden.
This study highlights and clarifies the substantial burden of AF and its implications for preparing efficacious AF management plans to address the imminent rise in prevalence.
本研究通过使用具有全国代表性的大型样本和匹配对照,更全面地考察成人房颤患者的疾病人文负担(生活质量、活动受限和医疗资源利用),从而在当前房颤和健康结局研究的基础上进一步推进。
本研究的数据来自基于互联网的 2009 年美国国家健康与健康调查。结果指标包括来自 SF-12 的心理健康和生理健康综合评分(MCS 和 PCS)和健康效用评分,以及活动受限、住院、医疗服务提供者和急诊室(ER)就诊。根据房颤和非房颤状态对患者进行年龄和性别匹配,各匹配 1296 例。使用广义线性模型,在控制 CHADS2 评分、合并症计数、人口统计学和临床变量的情况下,考察了房颤与非房颤状态对结果的影响。探索性结构方程模型在人文负担的综合模型中评估了上述结果。
房颤患者(来自 75000 名总样本中的 1296 名)的平均年龄为 64.9 岁,65.1%为男性。在调整了混杂因素后,与非房颤患者相比,房颤患者的 MCS、PCS 和效用评分较低,活动受限程度更高(比率比=1.26),传统医疗服务提供者就诊次数更多(比率比=1.43),ER 就诊和住院的可能性更高(OR=2.53 和 OR=2.71)。探索性结构方程模型分析表明,房颤患者的整体人文负担明显更高。
本研究强调并阐明了房颤的巨大负担,以及为制定有效的房颤管理计划以应对即将增加的患病率而做出准备的意义。