Wegner Christian, Hübner Nils-Olaf, Gleich Sabine, Thalmaier Ulrike, Krüger Colin M, Kramer Axel
Institute of Hygiene and Environmental Medicine, University Medicine Greifswald, Ernst-Moritz-Arndt University, Greifswald, Germany.
GMS Hyg Infect Control. 2013 Apr 29;8(1):Doc12. doi: 10.3205/dgkh000212. eCollection 2013.
Antibiotic resistance of bacterial pathogens is an emerging problem worldwide. To combat multidrug resistant organisms (MRDOs) networks of care providers have been established in all states in Germany. The HICARE-network, a project to combat MRDOs, founded by the Federal Ministry of Education and Research, has published data from 2010 of a voluntary, German-wide, multicenter point-prevalence survey in 2011 conducted in collaboration with the German Society of Hospital Hygiene. The aim of the present survey was the re-evaluation of the situation in 2012.
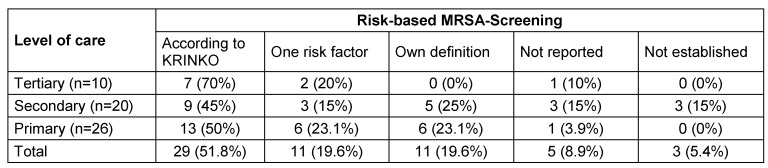
The survey was conducted as a voluntary, anonymous, point-prevalence in May 2012 using routine data of microbiological diagnostics of the hospitals. As in the former survey of 2010 it was differentiated between primary, secondary and tertiary care hospitals and only data from intensive care units, surgical and medical wards were collected. Based on the survey form used in 2010, an updated version was used including more pathogens and corrected issues observed in the former survey. Methicillin-resistant Staphylococcus aureus (MRSA) (total as well as separated in hospital-acquired (HA), community-acquired (CA) and lifestock-associated (LA) MRSA), vancomycin resistant Staphylococcus aureus (VRSA/GRSA), vancomycin resistant Enterococcus faecalis resp. Enterococcus faecium (VR-E. faecalis resp. VR-E. faecium), extended-spectrum-beta-lactamase-building (ESBL) E. coli (ESBL-EC) and Klebsiella pneumoniae (ESBL-KP), multiresistant Acinetobacter spp. (MAB), multiresistant Pseudomonas spp. (MRP), carbapenemase-producing Enterobacteriaceae (CRE) as well as Clostridium difficile (CD) infections and severe infections requiring ICU-treatment were included in the survey along with additional data on screening strategy, the equipment with infection control staff and possible confounders.
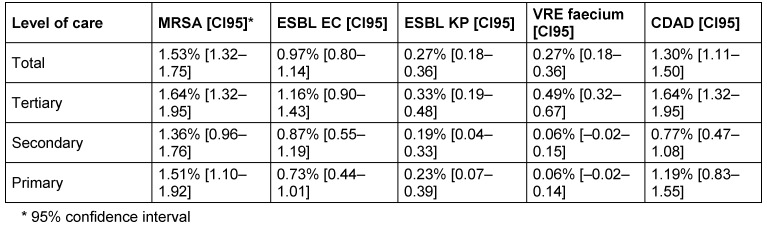
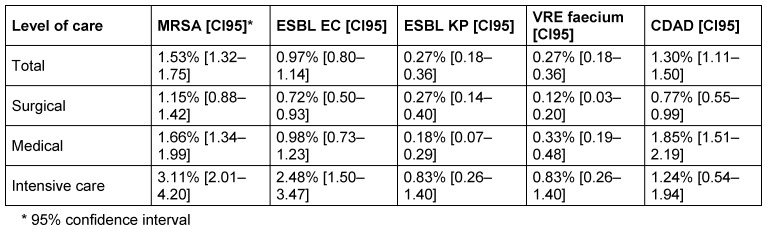
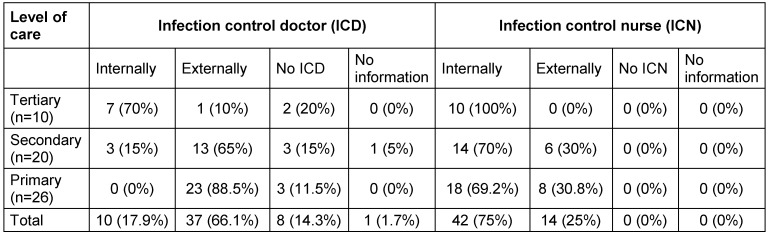
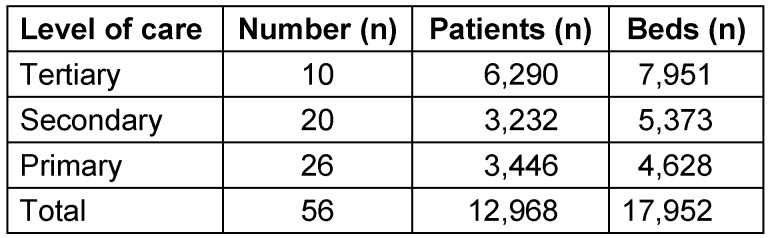
Out of 1,550 hospitals asked to participate, 62 returned data (4%). Data from 56 hospitals including primary (26), secondary (20) and tertiary (10) care hospitals were analyzable (3.6%). The most frequently reported organisms were MRSA 1.53% [CI95: 1.32-1.75], followed by CDAD 1.30% [CI95: 1.11-1.50], ESBL-EC 0.97% [CI95: 0.80-1.14], and ESBL-KP 0.27% [CI95: 0.18-0.36], regardless of the level of care. Prevalence of MRDOs depended on the level of care and on the type of ward, as expected. Overall prevalence was highest on intensive care wards, and prevalences were remarkably high on medical wards compared to surgical wards. All tertiary care providers employed their own infection control nurse, while only ~70% of the secondary and primary care hospitals did. Surprisingly, in two of the ten participating tertiary care providers neither an internal nor an external infection control doctor was available.
With more than 13,000 patients in 56 hospitals distributed all over Germany, the survey included more than three times as many patients as the first survey and therefore not only adds valuable information about the epidemiology of emerging nosocomial pathogens, but also helps to raise awareness of the problem of antibacterial resistance in Germany. The prevalences reported seem to be comparable to the results of the former survey and of other surveys published. Some hospitals reported to have no infection control personnel available at all. This statement is in line with another survey published in this issue.
细菌病原体的抗生素耐药性是全球范围内一个新出现的问题。为应对多重耐药菌,德国所有州都建立了医疗服务提供者网络。由联邦教育与研究部发起的抗击多重耐药菌项目HICARE网络,公布了2010年与德国医院卫生协会合作在德国范围内开展的一项自愿性多中心现患率调查的数据。本次调查的目的是重新评估2012年的情况。
本次调查于2012年5月以自愿、匿名的方式进行现患率调查,采用医院微生物诊断的常规数据。与2010年的前一次调查一样,区分了一级、二级和三级护理医院,仅收集重症监护病房、外科和内科病房的数据。基于2010年使用的调查问卷,使用了一个更新版本,包括更多病原体,并纠正了前一次调查中发现的问题。耐甲氧西林金黄色葡萄球菌(MRSA)(包括医院获得性(HA)、社区获得性(CA)和家畜相关(LA)MRSA的总数及分类)、耐万古霉素金黄色葡萄球菌(VRSA/GRSA)、耐万古霉素粪肠球菌或屎肠球菌(VR-E. faecalis或VR-E. faecium)、产超广谱β-内酰胺酶(ESBL)的大肠埃希菌(ESBL-EC)和肺炎克雷伯菌(ESBL-KP)、多重耐药不动杆菌属(MAB)、多重耐药假单胞菌属(MRP)、产碳青霉烯酶肠杆菌科细菌(CRE)以及艰难梭菌(CD)感染和需要重症监护治疗的严重感染均纳入调查,同时还包括关于筛查策略、感染控制人员配备及可能混杂因素的其他数据。
在被邀请参与的1550家医院中,62家返回了数据(4%)。来自56家医院的数据可进行分析,其中包括一级护理医院26家、二级护理医院20家、三级护理医院10家(3.6%)。最常报告的病原体是MRSA,为1.53% [95%置信区间:1.32 - 1.75],其次是艰难梭菌感染相关性腹泻(CDAD),为1.30% [95%置信区间:1.11 - 1.50],ESBL-EC为0.97% [95%置信区间:0.80 - 1.14],ESBL-KP为0.27% [95%置信区间:0.18 - 0.36],与护理级别无关。正如预期的那样,多重耐药菌的现患率取决于护理级别和病房类型。总体现患率在重症监护病房最高,内科病房的现患率相比外科病房显著较高。所有三级护理机构都配备了自己的感染控制护士,而二级和一级护理医院只有约70%配备了。令人惊讶的是,在参与调查的10家三级护理机构中有两家既没有内部也没有外部的感染控制医生。
本次调查涵盖了德国各地56家医院的13000多名患者,调查的患者数量是第一次调查的三倍多,因此不仅增加了关于新出现的医院病原体流行病学的有价值信息,也有助于提高德国对抗菌药物耐药性问题的认识。报告的现患率似乎与前一次调查及其他已发表调查的结果相当。一些医院报告称根本没有感染控制人员。这一说法与本期发表的另一项调查结果一致。